

You may be at one of several turning points. You've finished training and want your first substantive consultant post. You're established in the NHS but questioning whether the rota, caseload and on-call burden are sustainable. Or you've developed an interest in autism, ADHD, personality disorder work, or broader psychological assessment and you're wondering whether the most suitable role now sits partly outside the traditional trust structure.
That uncertainty is normal. Psychiatry in the UK no longer offers one obvious career lane that suits everyone. Some doctors want a clear NHS progression with teaching, management and tribunal work. Others want sessional flexibility, a narrower specialist caseload, or a better balance between assessment work and ongoing treatment. Many want both.
What matters is understanding the trade-offs. A job title alone tells you very little. Two consultant psychiatrist posts can look similar on paper and feel entirely different in practice once you factor in legal responsibilities, admin support, waiting-list pressure, multidisciplinary team quality, and whether the service has enough doctors to run safely.
The Modern Psychiatrist's Career Crossroads
The modern psychiatrist has more options than the previous generation, but more choice also means more room for poor decisions. Junior colleagues often ask which path is “best”. That isn't the right question. The better question is which setting fits the kind of clinician you are, the kind of work you want to be known for, and the life you want outside medicine.

Some psychiatrists thrive in complex NHS systems where leadership, safeguarding, risk management and service development are part of the appeal. Others prefer focused diagnostic work, tighter clinical boundaries and less institutional friction. Neither is more serious or more ethical. They are different forms of psychiatric practice.
What usually sits behind the job search
In real life, most job searches are driven by one of these pressures:
- Training progression: You need the next post that strengthens your route to consultant practice.
- Service fatigue: You can do the work, but the current service model is draining your energy.
- Special interest development: You've found your niche in ADHD, autism, liaison, forensic, old age, CAMHS, or personality disorder work.
- Lifestyle change: Family commitments, commuting burden, portfolio working, or health reasons mean the old arrangement no longer fits.
- Professional identity: You want a role that reflects what you do well, not just what your current service needs.
There's also confusion around role boundaries, especially for patients and newer doctors moving into assessment-heavy services. If you need a concise explanation of that distinction, the guide on the difference between psychologist and psychiatrist in the UK is useful background, particularly when you're considering jobs that sit alongside clinical psychology and structured assessment teams.
Practical rule: Don't choose your next post by employer prestige alone. Choose it by daily work pattern, legal responsibility, supervision quality and whether the caseload matches your expertise.
The career question that matters
By this stage of the profession, the central question isn't “Can I get a psychiatry job?” It's “Which version of psychiatric practice will still suit me in three years?”
That's where many doctors go wrong. They focus on headline salary, job title, or geography, and ignore the design of the role itself. In 2026, jobs for psychiatrists in the UK aren't scarce in the broad sense. The challenge is sorting the sustainable posts from the draining ones, and separating genuine specialist work from generic vacancy filling.
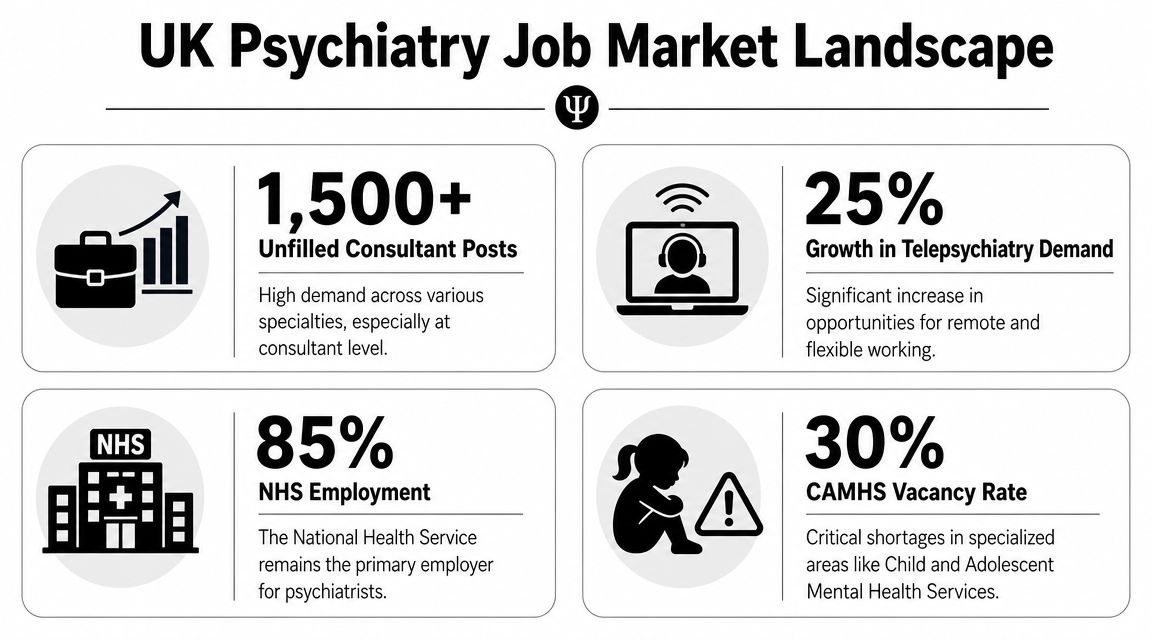
The UK Psychiatry Job Market Landscape
A psychiatry job advert in the UK can look reassuring on paper. Consultant title, decent salary, supportive team, flexible working. Then you speak to the service and find a six-month wait for admin support, repeated consultant gaps, and a caseload built around work you did not train for. That difference between advert and day-to-day practice matters more in psychiatry than in many other specialties.
Psychiatry remains a shortage market rather than a specialty that rises and falls with a routine hiring cycle. In England, the NHS had around 5,000 full-time equivalent consultant psychiatrists and vacancy rates of around 9%, according to the July 2023 workforce position described in this review of psychiatrist demand and NHS workforce planning. The practical implication is straightforward. Many employers are recruiting because services have been carrying unmet need for years, not because a single consultant has moved on.
That pressure creates opportunity, but it also creates noise. A shortage market produces good posts, mediocre posts, and posts that survive only because there is always another applicant willing to tolerate poor design for a year. Junior doctors and newly appointed consultants often underestimate that distinction.
The NHS still anchors the profession, but the market is no longer defined by NHS vacancies alone. Independent inpatient work remains established. What has changed more sharply is the expansion of assessment-led private services, particularly in ADHD and autism. That growth has created a different kind of role for psychiatrists: fewer ward pressures, more structured diagnostic work, faster report turnaround, and a heavier emphasis on consistency, documentation, and clear multidisciplinary boundaries. For some doctors, that is a better fit than a traditional community or inpatient consultant post. For others, it becomes repetitive quickly unless it sits inside a broader portfolio.
This is where career strategy matters. A doctor with strong general adult experience, Section 12 approval, and tribunal confidence may still choose a neurodevelopmental private post if they want predictable sessions and focused assessment work. A doctor who values longitudinal care, service leadership, and trainee supervision may find the same role too narrow after twelve months. Services such as Insight Diagnostics Global appeal to psychiatrists who want high-demand neurodevelopmental work within a defined assessment model, but that model suits clinicians who are comfortable with pace, standardisation, and report accountability.
What shortage actually changes for candidates
A tight hiring market gives good candidates more room to ask hard questions before accepting an offer. Use that room properly.
Ask about:
- Rota design: How often are you on call, and what does the actual overnight burden look like?
- Consultant establishment: Are you joining a staffed service or covering chronic vacancies?
- Caseload shape: Is the work mainly acute risk management, long-term follow-up, or assessment and diagnosis?
- Administrative capacity: Who handles letters, tribunal bundles, screening correspondence, and report formatting?
- Clinical boundaries: Are you being hired for your subspecialty skills, or to absorb whatever the service cannot otherwise cover?
- Time to start safely: How quickly can IT access, clinic templates, prescribing systems, and induction be put in place?
Those questions are not box-ticking. They tell you whether the post is sustainable.
Read the service, not just the advert
Job descriptions rarely say, “We have been short for two years and need someone to hold the line.” You infer that from the wording, the interview answers, and who turns up to meet you. If an employer talks constantly about flexibility and resilience but stays vague on consultant numbers, middle-grade support, and protected SPA time, I would treat that as a warning sign.
The same applies in the private sector. An ADHD or autism assessment role can be excellent work if pathways are clear, screening is done properly, admin is competent, and expectations around report turnaround are realistic. It can also become high-volume production medicine if the service is built around throughput rather than clinical quality. Ask who triages referrals, how complexity is filtered, what happens with borderline cases, and how prescribing responsibility is managed after diagnosis.
Pay still matters, of course, and doctors comparing sectors should understand the factors that drive it. This guide to how much psychiatrists make across NHS and private settings is a useful reference point. I would still rank workload design, legal exposure, and case mix above headline income.
A well-paid post with unclear boundaries, weak medical staffing, and unsafe cross-cover is still a poor job.
Navigating Core Psychiatry Pathways in the UK
For most psychiatrists, the backbone of a UK career still runs through structured postgraduate training, specialist accreditation and consultant practice. Even if you later move into independent or mixed-sector work, the credibility of that pathway matters. It signals not just seniority, but readiness for autonomous responsibility.
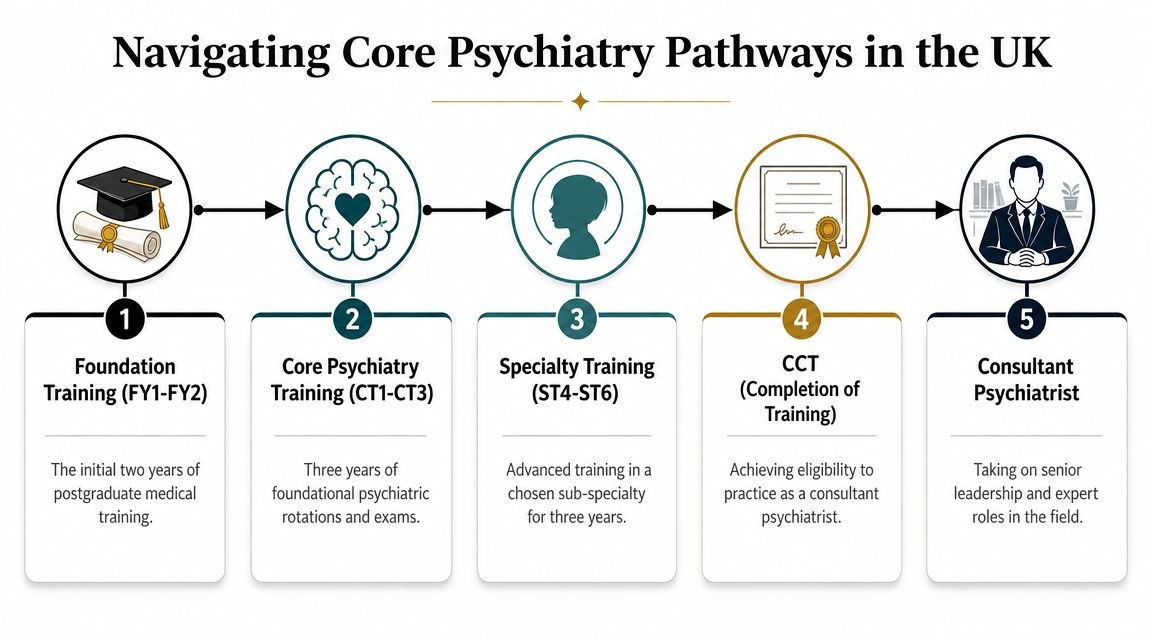
The usual ladder remains familiar: foundation training, core psychiatry training, higher specialty training, completion of training, then substantive or locum consultant work. That outline is simple. What trips people up are the gatekeeping credentials that determine what you can do once appointed.
The credentials that change employability
The key bottleneck for many UK roles is the GMC Specialist Register plus Section 12 approval for Mental Health Act work. NHS and independent providers commonly treat these as hard requirements because they affect whether you can independently assess detention criteria, authorise treatment pathways and manage statutory documentation. That directly affects hiring speed and eligibility for consultant-level posts, as discussed in this summary of the credentialing bottleneck for psychiatrist roles.
In practical terms:
- Specialist Register: Essential for mainstream consultant eligibility.
- Section 12 approval: Often decisive for inpatient, crisis, tribunal and other MHA-facing roles.
- Subspecialty experience: This shapes not just appointment chances, but what kind of post you're offered.
- References and appraisal evidence: These matter more than many trainees realise when a service needs quick appointment but still needs confidence in governance.
If you lack one of the formal requirements, it doesn't mean your options disappear. It does mean your route may be through SAS, associate specialist, trust-grade or transitional roles while you complete the missing credential.
NHS consultant track versus locum track
There's no single correct answer here. The better choice depends on what you need from the next two or three years.
| Path | Usually suits | Main strengths | Main cautions |
|---|---|---|---|
| Substantive NHS post | Doctors wanting stability, team identity, pension and service leadership | Continuity, influence, training roles, established MDT links | Can bring persistent admin load and fixed organisational pressures |
| Locum consultant work | Doctors wanting flexibility, varied settings or interim income planning | Control over commitments, quicker movement between roles | Less continuity, weaker institutional belonging, variable support |
| SAS or specialist doctor route | Doctors building UK experience or shaping a non-traditional path | Strong clinical exposure, progression options, practical route into services | Scope may be narrower where statutory responsibilities are restricted |
A common mistake is to treat locum work as either purely opportunistic or somehow less serious. Good locum practice can be highly professional and clinically valuable. Poorly chosen locum work, however, leaves doctors carrying someone else's unresolved staffing problem.
Before you decide, it helps to hear how the training pathway is typically described in straightforward terms. This overview is a useful primer:
What works and what doesn't
What works is sequencing your career deliberately. Get the essential approvals in order. Build a reputation in one or two areas rather than presenting yourself as a generic pair of hands. Choose early consultant roles where supervision, cover and administrative systems are visible.
What doesn't work is assuming all consultant posts are interchangeable, or that a prestigious trust automatically offers a better working life. In psychiatry, your effectiveness depends heavily on the system around you. A well-supported district service can be a better first consultant post than a famous but chaotic one.
Specialising in High-Demand Fields and Private Practice
The most interesting shift in jobs for psychiatrists isn't merely that there are vacancies. It's that specialist assessment work has become a distinct career lane in its own right, especially in adult ADHD, autism and broader mental health assessment. Many psychiatrists discover a different style of practice within this area. The work is still clinically demanding, but the rhythm can be more deliberate, the reporting more structured, and the patient journey clearer.
That change matters because many doctors are no longer choosing between “NHS” and “private” as if one must cancel the other out. Increasingly, they build mixed careers. A consultant might retain NHS commitments for complex risk work, leadership or teaching, while adding sessional private assessment work in neurodevelopmental conditions or personality-related diagnostic clarification.
Why neurodevelopmental assessment has become a serious niche
Adult ADHD and autism assessments require more than enthusiasm for the topic. Good services need careful triage, structured interviews, collateral history where available, differential diagnosis, attention to trauma and personality factors, and a disciplined approach to diagnostic thresholds. The psychiatrist who does this well combines medical formulation with psychological mindedness.
That's one reason consultant-led private services have drawn interest from experienced clinicians. The work can be narrower than general community psychiatry, but not easier. You need to be comfortable distinguishing overlapping presentations such as anxiety, mood instability, trauma, sleep-related impairment, substance misuse, autistic traits, attentional symptoms and enduring personality features.
Doctors who are particularly strong in this area often bring one or more of the following:
- Structured assessment confidence: They can conduct long diagnostic interviews without becoming vague or over-inclusive.
- Report-writing discipline: Their reports are clear, defensible and useful to patients, GPs and other clinicians.
- Comorbidity awareness: They don't diagnose ADHD or autism in isolation from depression, anxiety, bipolarity, trauma or personality disorder.
- Treatment follow-through: They understand what happens after diagnosis, including psychoeducation, medication discussions where relevant, signposting and shared care considerations.
What a private specialist role can offer
A well-run private clinic can suit psychiatrists who want to practise with tighter boundaries and greater focus. The attraction is not solely independence. It's the chance to work in a service model where assessment length, admin time and multidisciplinary contribution are thought about in advance.
That matters because the central job question isn't only where vacancies exist. It's whether the service is staffed and organised safely. Roles are often more attractive in services, including private clinics, that can show protected admin time, multidisciplinary support and realistic appointment volumes, which directly addresses burnout risk, as noted in this discussion of staffing safety and caseload quality.
The best private work isn't the fastest work. It's the work done in a setting where diagnostic care remains careful, reports are given proper time, and the doctor isn't pushed to sacrifice judgement for throughput.
Models of private engagement
Private practice isn't one thing. A psychiatrist may work in several ways at once:
- Sessional associate work: You take defined clinics or assessment sessions, often with central admin support.
- Portfolio consultant practice: You combine NHS, medico-legal, teaching and assessment roles.
- Full-time independent sector role: Less common, but attractive to some doctors who prefer specialist service design over broad trust commitments.
There's particular value in clinics that understand both neurodevelopmental and general mental health presentations. In adult services, straightforward diagnostic stories are the exception, not the rule. Many patients present after years of misunderstanding, partial treatment, burnout or academic and occupational difficulties. A psychiatrist who can hold the whole picture, including personality structure and functional impact, is far more useful than one who applies labels mechanically.
For clinicians exploring this area, it's worth looking at how private psychiatrist assessment pathways are structured in modern consultant-led services. This overview of a private psychiatrist assessment gives a practical sense of what patients and referrers increasingly expect.
Other high-demand subspecialties worth considering
Neurodevelopmental work is not the only route. In the current UK context, doctors with strong fit in CAMHS, learning disability, forensic, old age and liaison psychiatry remain highly attractive to employers. Those fields reward clarity, risk competence and resilience, but they differ sharply in day-to-day life.
A few blunt observations help:
- If you enjoy legal process and complex boundaries, forensic work may suit you.
- If you like interface work and fast formulation, liaison can be deeply satisfying.
- If you value family systems and developmental thinking, CAMHS remains compelling.
- If you want medicine and psychiatry to speak to each other daily, old age and liaison often provide that richness.
The mistake is chasing “high demand” alone. A subspecialty becomes a sustainable career only when your temperament fits the work.
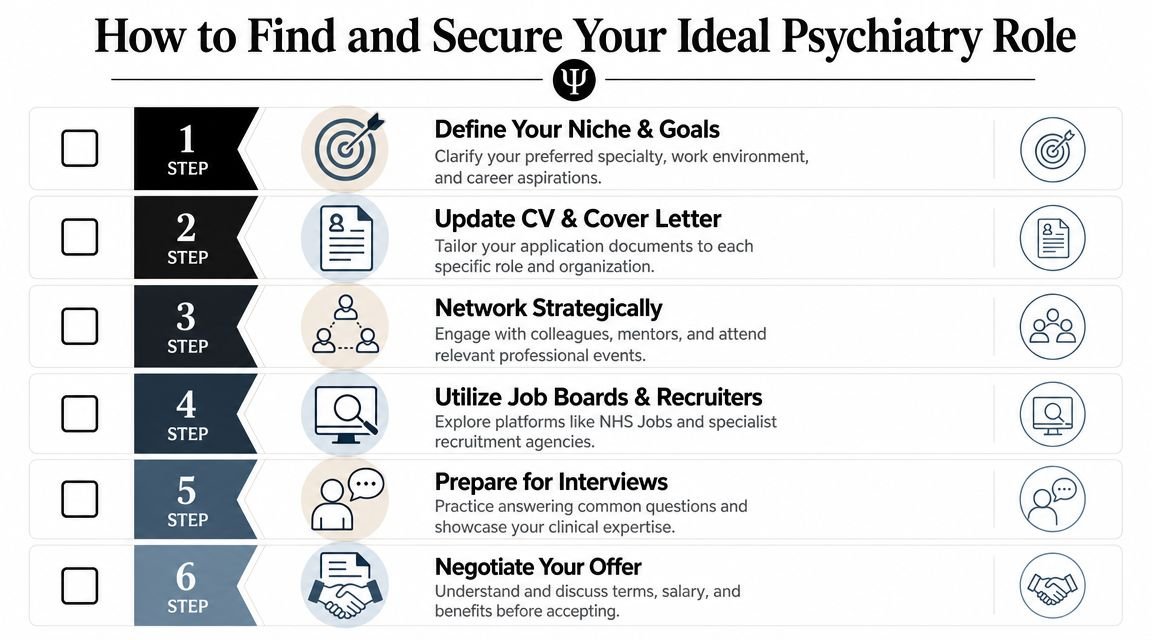
How to Find and Secure Your Ideal Psychiatry Role
Once you know what kind of practice you want, the job hunt becomes simpler. Not easy, but simpler. The strongest candidates aren't always the most decorated. They're usually the ones who present a coherent story: this is my expertise, this is the work I'm ready for, and this is how I'll contribute safely from day one.
Where to look
Use several channels at once. Relying on a single jobs board is a weak strategy.
- NHS Jobs: Still the default place for substantive and many trust-grade posts.
- Specialist agencies: Useful for locum and interim consultant work, though quality varies.
- Professional network: Previous supervisors, college contacts and ex-colleagues often know about roles before formal listing.
- LinkedIn and direct approaches: Particularly relevant for independent providers and assessment services.
If you're considering private or mixed-sector work, look at service design, governance, clinic flow and who is supervising clinical standards. A polished website isn't enough.
How to tailor your CV properly
Psychiatry CVs often fail because they read like generic medical CVs. Employers don't need a broad autobiography. They need evidence that you can solve the problem they are hiring for.
UK psychiatrist job demand is constrained by workforce supply, and employers compete on rota stability and subspecialty fit. Candidates with experience in CAMHS, learning disability, forensic or liaison psychiatry often have stronger placement options because services use those skills to reduce rota gaps and keep waiting lists moving, which directly affects how a CV should be adapted, as noted in this analysis of psychiatry hiring pressure and subspecialty fit.
That means your CV should foreground the right things early:
- Regulatory status first. Put GMC registration, Specialist Register status and Section 12 approval near the top.
- State your niche clearly. General adult with ADHD assessment experience is different from liaison with tribunal exposure or old age with dementia pathway leadership.
- Show operational competence. Mention tribunal work, MHA assessments, diagnostic reporting, risk management, teaching, service development or prescribing follow-up where relevant.
- Be concrete about assessment tools and methods. If you work in neurodevelopmental assessment, list structured approaches and relevant clinical experience rather than making vague claims about “specialist interest”.
- Cut irrelevance. Detailed audit descriptions from years ago won't compensate for missing present-day role fit.
Interview performance that actually changes outcomes
Psychiatry interviews often turn on judgement rather than charisma. Panels want to know whether you are safe, thoughtful and manageable in a pressured service.
Prepare for questions in these areas:
- Clinical ambiguity: How do you handle overlapping diagnoses or uncertain formulation?
- MHA and legal judgement: Can you explain your decision-making under pressure?
- Service pressure: What do you do when demand exceeds immediate capacity?
- Teamwork: How do you use psychologists, nurses, occupational therapists and support staff effectively?
- Boundaries: Can you describe what you would and would not take on in the role?
Interview advice: Panels remember candidates who answer difficult questions calmly, define limits clearly, and avoid pretending to know what they don't know.
For doctors applying to specialist services, keep examples ready from real work. A strong answer about a complex ADHD differential, an autism assessment complicated by trauma history, or a patient with personality vulnerabilities and mood instability will carry more weight than polished generalities.
If you're actively exploring openings in specialist assessment teams, it's sensible to watch current psychiatry opportunities and team openings alongside the usual NHS routes.
Your Next Steps in Your Psychiatry Career
You finish clinic on a Friday with two offers on the table. One is a standard NHS consultant post with a heavy community caseload, on-call commitments and a clear route into local leadership. The other is a specialist assessment role with tighter boundaries, more diagnostic depth and less crisis work. Both are respectable jobs for psychiatrists. They will produce very different working weeks, different clinical risks and different long-term careers.
That is the decision point that matters now. The question is not whether psychiatry offers security. As noted earlier, it does. The main question is what kind of psychiatrist you want to be over the next five years, and which setting will let you do good work without burning through your judgement, patience or health.
A sensible plan for the next month
- Set your priority clearly. Decide whether you want stability, sub-specialist development, autonomy, better boundaries, income growth, or a portfolio career. Rank them.
- Check your practical readiness. Review your appraisal record, references, Section 12 approval, prescribing history, indemnity position and Specialist Register status before sending applications.
- Tailor your CV to the post. If you want ADHD, autism or diagnostic assessment work, bring that experience to the top. Do not lead with generic service duties and expect the panel to infer your interest.
- Test the service, not just the title. Ask who triages referrals, how much admin falls to the psychiatrist, what happens with risk escalation, how reports are quality-checked and whether the MDT functions effectively.
- Compare NHS and private work thoroughly. NHS posts usually offer stronger structure, pension benefits, training exposure and easier peer support. Private specialist services can offer cleaner assessment pathways, more control over pace and higher earning potential, but they also expect efficiency, clear documentation and sound boundary management.
- Prepare your account of yourself. You need a short, credible explanation of why you are moving, what you do well, and which conditions help you practise safely at a high standard.
I usually tell trainees and new consultants to choose for fit, not for prestige.
A doctor who works well in a pressured CMHT may feel constrained in a private assessment model. Another may produce better formulations, better reports and better patient experience in a focused neurodevelopmental service than in a post dominated by crisis containment and bed pressure. Neither path is automatically better. The trade-off is between breadth and focus, between system responsibility and personal control, and between institutional progression and portfolio flexibility.
That trade-off has become more important as private work in adult ADHD and autism has expanded. Some of these roles are poorly designed and reduce the psychiatrist to rapid throughput. Some are well-run and give proper time for collateral history, differential diagnosis, report writing and follow-up. Junior doctors often underestimate how much this operational detail affects job satisfaction. A service with a clear pathway, sensible admin support and defined clinical thresholds can be a better long-term move than a more famous post with chaotic demand.
It also helps to sharpen the non-clinical side of applications. If you want a practical resource on presenting your value without sounding rehearsed, this guide on how to sell yourself in an interview is worth reading before consultant or specialist-role applications.
If you are considering specialist private or mixed-model work, look closely at providers that have built a serious assessment structure rather than a referral funnel. Insight Diagnostics Global is one example worth reviewing for psychiatrists interested in adult ADHD, autism and broader mental health assessment. Their model includes online and face-to-face adult assessments, GMC Specialist Register psychiatrists, structured diagnostic pathways and follow-up options including ADHD titration. For the right clinician, that kind of service offers a distinct career proposition. Less crisis work, more diagnostic precision, and a chance to build expertise in an area where demand is still rising.
Good psychiatry careers are chosen with intention. Pick the setting that matches your judgement, your tolerances and the kind of clinical work you want to be known for.