

You've finally got an explanation for years of missed deadlines, mental overload, abandoned routines, and the odd feeling that life has always been harder than it looked for other people. An adult ADHD diagnosis often brings relief first, then a very practical question soon after: which medication should I start with?
For many adults in UK practice, that decision comes down to methylphenidate or lisdexamfetamine. Both are established first-line stimulant options. Both can work very well. Neither is automatically the “best” choice just because it performed slightly better in one study or because a friend felt calmer on it.
What matters is fit. The right medication is the one that improves attention, task initiation, working stamina, and emotional regulation without creating side effects that make daily life harder. That becomes even more important when ADHD sits alongside autism, anxiety, low mood, trauma history, burnout, or sensory sensitivity. In those cases, the medication's “feel” matters almost as much as its effect.
Starting Your ADHD Medication Journey
A common scenario in clinic goes like this. Someone reaches adulthood carrying years of effort, shame, and masking. They've built systems, broken systems, changed jobs, blamed themselves, and still felt unable to do simple things consistently. Then they receive an ADHD diagnosis and start looking at treatment options.
The next question is usually immediate. What now? If medication is appropriate, the first discussion often centres on methylphenidate products such as Ritalin or Concerta XL, and lisdexamfetamine, commonly known in the UK as Elvanse. If you're trying to understand the practical route into treatment, this guide on how to get ADHD medication in the UK is a useful starting point.
The decision isn't about a winner
Patients often come in asking for the stronger one, the smoother one, or the one “with fewer side effects”. That's understandable, but it oversimplifies the decision. In real clinical work, the more useful question is this:
Which medication is most likely to suit your nervous system, your routine, and your co-occurring conditions?
For one person, that means all-day coverage for work, commuting, and family life. For another, it means avoiding an edgy or overstimulated feeling because they're also autistic and highly sensory-sensitive. For someone else, it means having enough flexibility to cover only part of the day.
A quick comparison
| Feature | Methylphenidate (e.g., Concerta, Ritalin) | Lisdexamfetamine (Elvanse) |
|---|---|---|
| Drug class | Stimulant | Stimulant |
| How it works | Primarily blocks reuptake of dopamine and noradrenaline | Prodrug converted to dexamfetamine, increasing neurotransmitter release and also affecting reuptake |
| Formulation options | Immediate-release and modified-release forms | Long-acting formulation |
| Practical strength | Flexibility | Longer, steadier coverage for many adults |
| Typical choice factors | Need for adjustable timing, shorter coverage, stepwise titration | Need for long workday coverage, smoother profile for some patients |
| Best option overall | Depends on response and tolerability | Depends on response and tolerability |
How These Medications Work Differently
The broad aim is the same. Both medications increase the availability of dopamine and noradrenaline, which helps with attention, task persistence, impulse control, and mental organisation. The difference lies in how they do it.
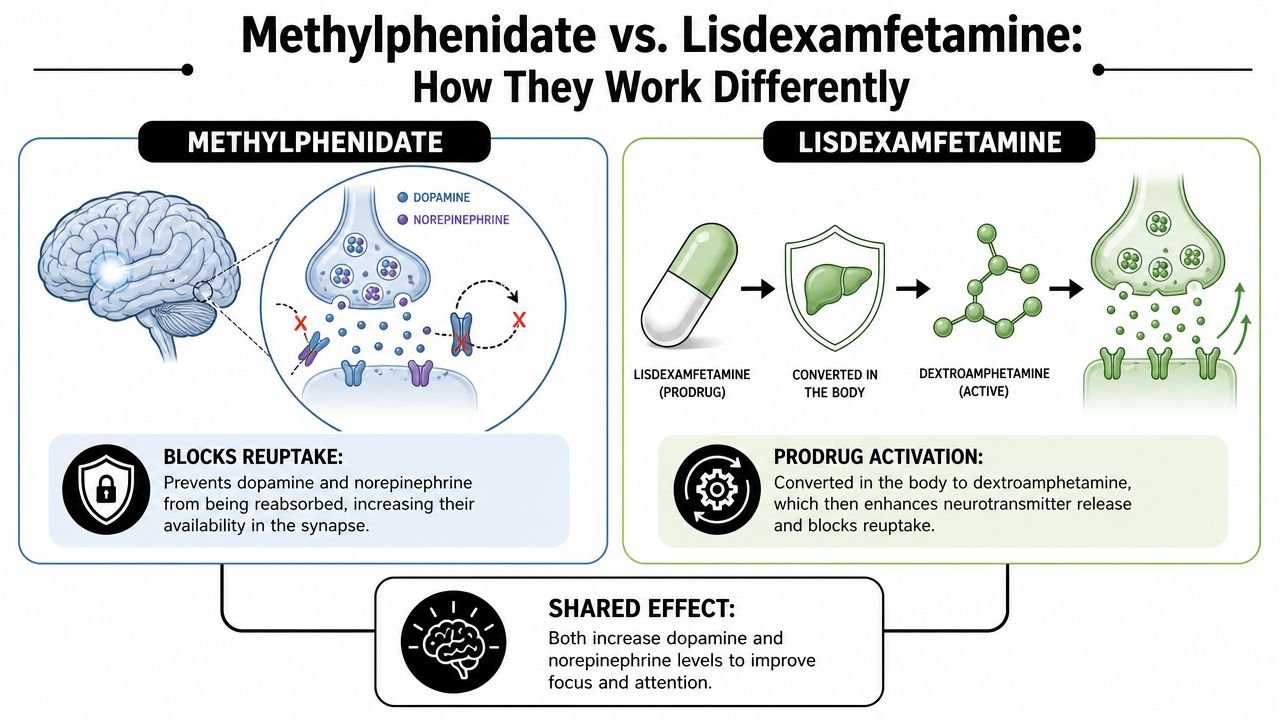
Methylphenidate blocks reuptake
A simple analogy helps. Think of brain messaging like a post room. Chemical messengers are sent out between nerve cells, carry information, then get taken back up after use. Methylphenidate mainly works by blocking that return process, so more of those messengers stay active for longer.
That's why many people describe methylphenidate as helping them feel more able to start, sustain, and complete tasks without necessarily feeling dramatically different in themselves.
Lisdexamfetamine is a prodrug
Lisdexamfetamine starts off inactive. Your body converts it into dexamfetamine after absorption. Once active, it increases neurotransmitter availability in a different way, including promoting release.
In practice, some adults experience this as a smoother build rather than a quick “kick”. Others notice that it lasts through more of the day.
For a broader overview of stimulant treatment options, this explainer on stimulant ADHD medication is a good companion read.
A visual summary can make this easier to grasp:
Why mechanism matters in real life
The mechanism doesn't just matter to pharmacologists. It often shapes the lived experience of treatment.
- Onset experience: One medication may feel more gradual, while another feels more noticeable when it starts.
- Wear-off pattern: Some patients are very sensitive to the end-of-dose period. That can affect mood, appetite, and evening functioning.
- Sensory profile: Autistic adults sometimes report that one stimulant feels clearer and calmer, while the other feels more physically present or “buzzier”.
- Dose adjustments: The way the medication is formulated changes how precisely a prescriber can adjust timing and coverage.
In clinic, the medication that looks ideal on paper isn't always the one a patient stays on. The subjective feel matters.
Comparing Formulations Onset and Duration
The methylphenidate vs Lisdexamfetamine discussion becomes practical rather than theoretical. Most adults don't care how elegant the mechanism sounds. They care whether they can work, eat, sleep, parent, study, drive, and ultimately recover.
Methylphenidate gives more formulation choice
Methylphenidate comes in immediate-release and modified-release forms. That gives clinicians more room to tailor treatment around a person's routine.
Immediate-release preparations can be useful when you want:
- Shorter coverage
- More precise control over timing
- A cautious start for someone sensitive to medication
- A way to test response before moving to longer-acting forms
Modified-release forms are often chosen when the goal is a more convenient once-daily option with steadier daytime coverage.
Lisdexamfetamine tends to feel more all-day
Lisdexamfetamine is used as a long-acting option. In the adult discussion summarised in a comparative review, long-duration effects in the 12.5 to 14 hour range were noted, which helps explain why many working adults consider it when they need coverage beyond standard office hours (adult comparative review).
That doesn't mean longer is always better. Some adults love the endurance. Others find they don't want medication effects stretching too far into the evening.
Daily-life examples
A few patterns come up repeatedly in practice.
| Situation | Methylphenidate may suit | Lisdexamfetamine may suit |
|---|---|---|
| Variable schedule | Yes, especially if timing needs to change | Less flexible in timing |
| Long workday | Sometimes, depending on formulation | Often a strong option |
| Sensitive to “peaks” | Depends on formulation and person | Some people find it smoother |
| Wants a shorter trial window | Often easier | Less ideal |
| Evening responsibilities | May need planning around duration | Often helpful if long coverage is needed |
If you're trying to match medication timing to your day, this guide on how long ADHD medication takes to work can help frame the discussion.
What doesn't work well
Some assumptions create problems early on.
- Choosing purely by brand reputation: A well-known name tells you very little about how your own body will respond.
- Ignoring routine: A medication can be clinically sound and still fail because it doesn't fit your work hours, eating pattern, or sleep cycle.
- Overvaluing the first day: Early impressions matter, but they don't settle the question. The first few days can be misleading.
- Treating side effects as a sign to push through anything: Mild settling effects can happen. Ongoing distress, marked anxiety, or intolerable appetite suppression shouldn't be brushed aside.
A Look at the Evidence on Efficacy
A common clinic scenario is this: one adult patient wants the medication with the strongest chance of symptom improvement, while another wants the option that is easiest to adjust around work, sleep, meals, and co-occurring autism or anxiety. The evidence helps, but it does not settle the prescription on its own.
What head-to-head studies show
One often-cited comparison looked at 336 randomised patients and found higher response rates with lisdexamfetamine than with OROS methylphenidate, with 74.2% meeting the prespecified response threshold at endpoint versus 55.9%, compared with 10.7% for placebo. The same analysis reported least-squares mean ADHD-RS-IV reductions of −24.3 for lisdexamfetamine, −18.7 for OROS methylphenidate, and −5.7 for placebo (head-to-head analysis in PMC).
That result matters, but it needs context. It compares specific formulations in a trial setting. In UK adult practice, we are rarely deciding between abstract drug classes. We are choosing between a particular formulation, a specific dose range, and a patient with a real routine, real comorbidity, and a real threshold for appetite loss, insomnia, irritability, or rebound.
The broader NICE-linked picture
The more useful reading for UK practice is broader and more restrained. In a UK-focused evidence summary prepared alongside NICE guidance, adolescent comparator studies found that lisdexamfetamine produced a larger reduction in ADHD-RS-IV scores than osmotic-release methylphenidate in one forced-dose trial, with mean change −25.6 versus −23.5, and lisdexamfetamine was statistically superior on ADHD-RS-IV total score and CGI-I in that design. In the flexible-dose trial, both treatments remained highly effective versus placebo, and the paper concluded that either stimulant class can be used with confidence. The same article reported efficacy effect sizes ranging from −0.43 to −1.16 versus placebo (UK-focused NICE evidence summary).
That is closer to how specialists interpret the evidence.
What I take from that in adult ADHD care
Lisdexamfetamine may show a modest average advantage in some datasets. Methylphenidate remains a strong first-line option. The clinically important point is that group averages do not predict an individual response well enough to choose on efficacy tables alone.
This becomes even more relevant in adults with co-occurring conditions. In an autistic adult, for example, a medication that looks slightly stronger on a rating scale may still be the wrong first choice if the person is highly sensitive to appetite suppression, physical tension, or a long duration they cannot easily switch off in the evening. In another patient with long work hours and frequent late-afternoon drop-off, lisdexamfetamine may be the more practical choice even if both classes are reasonable on paper.
For that reason, specialist clinics such as Insight Diagnostics do not treat this as a simple "which is better" question. We use the evidence to narrow the options, then match the medication to the patient in front of us.
If you want a practical explanation of how psychiatrists judge whether ADHD medication is working, that overview is useful.
A final practical point. Response is easier to judge when food intake, hydration, and timing are stable enough that we are not mistaking under-eating or late-day crashes for medication failure. Some adults find that simple planning around meals makes titration much clearer, and these nutrition strategies for ADHD can support that process.
Methylphenidate vs Lisdexamfetamine at a glance
| Feature | Methylphenidate (e.g., Concerta, Ritalin) | Lisdexamfetamine (Elvanse) |
|---|---|---|
| Evidence position | Strong first-line option | Strong first-line option |
| Comparative efficacy | Highly effective, sometimes slightly lower on average in some direct comparisons | Highly effective, sometimes slightly stronger on symptom scales |
| Clinical reading | A good option if flexibility, shorter coverage, or cautious adjustment matters | A good option if sustained coverage and consistent effect matter more |
| Best interpretation | Choose based on response, tolerability, routine, and comorbidity | Choose based on response, tolerability, routine, and comorbidity |
Side Effects and Safety Monitoring
The side-effect conversation should be calm and specific. Both medications can be very helpful. Both can also cause problems if they're a poor fit or if monitoring is loose.
Common issues clinicians watch for
The overlap is substantial. In routine practice, the main concerns are usually:
- Appetite reduction: Some adults eat less without realising it, then feel wired, flat, or irritable later in the day.
- Sleep disturbance: This can happen if the dose is too high, starts too late, or lasts longer than your day requires.
- Dry mouth and physical tension: Often manageable, but worth watching.
- Pulse and blood pressure changes: These need proper baseline assessment and follow-up.
- Anxiety or irritability: Sometimes the medication unmasks pre-existing anxiety. Sometimes it's just the wrong stimulant for that person.
A useful support alongside medication is practical habit support around meals and routine. Adults who lose appetite early in titration often benefit from planning food deliberately, and these nutrition strategies for ADHD can help make that easier.
Side effects aren't just a checklist
The same side effect can mean different things in different patients. “I feel anxious” might mean the dose is too strong. It might mean the medication is wearing off badly. It might mean the person had unmanaged anxiety all along, and improved focus has made them more aware of it.
For autistic adults, I pay particular attention to the texture of the response. Some describe a useful clarity. Others feel physically activated in a way they find intrusive. That's clinically important, even if the textbook side effects look mild.
A medication isn't successful just because concentration improves. It has to leave the person more functional overall.
Monitoring should be structured
Good prescribing includes a before-and-after comparison, not just a prescription pad.
A sensible monitoring process usually includes:
- Baseline review of physical health, pulse, blood pressure, current medication, and mental health history.
- Early follow-up after starting or changing dose.
- Ongoing review of benefit, appetite, sleep, mood, and physical effects.
- Adjustment or switch if the balance is wrong.
What doesn't work is starting a stimulant and then hoping for the best. Titration should be active. The dose, formulation, and sometimes even the medication class need refinement.
How We Make the Choice in Clinical Practice
A typical adult seen in a UK specialist clinic is deciding between these medications while also trying to hold down work, protect sleep, manage anxiety, and make sense of traits that may reflect autism as well as ADHD. In that setting, the question is rarely “which is better?” The better question is which option is more likely to help in real life, with side effects and daily demands taken seriously from the start.
In practice, I choose between methylphenidate and lisdexamfetamine by looking at the whole pattern, not just headline efficacy. Adults do not present with ADHD in a vacuum. They often come with sensory sensitivity, panic symptoms, depressive episodes, obsessive traits, chronic insomnia, burnout, or a long history of feeling overstretched by ordinary demands. Those details change prescribing.
For autistic adults, this matters even more. Two patients can report similar improvement in attention, but one may describe a calmer, cleaner effect, while the other feels physically driven or uncomfortable in their body. That difference affects adherence. It also affects whether the medication is effectively helping function, relationships, and recovery from day-to-day strain.
Certain patterns come up often in clinic:
- Autism with sensory sensitivity: a smoother subjective effect and a gentler wear-off may matter more than raw duration.
- Anxiety or panic vulnerability: slower titration and careful dose selection usually matter more than choosing the strongest effect.
- Irregular schedules or shift-based work: methylphenidate can be useful when formulation flexibility is part of the goal.
- Long workdays with evening responsibilities: lisdexamfetamine may suit adults who need steadier coverage across the day.
The first prescription is a starting point, not a verdict.
As noted earlier in the comparative discussion, much of the useful decision-making happens after the first medication does not work well enough, or works but feels wrong. In adult practice, I often learn more from the quality of that first response than from the baseline symptom list. Did attention improve but appetite collapse? Did motivation improve but the patient feel tense, flat, or overly activated? Did the benefit fade too early, or continue into the evening and disrupt sleep? Those answers usually tell me whether to adjust the dose, change the formulation, or switch stimulant class.
The aim is not to defend the first choice. The aim is to find the treatment you can function well on over time.
A practical framework helps:
| Clinical question | Why it matters |
|---|---|
| How long do you need symptom coverage on a normal day? | This helps decide whether flexibility or longer duration is the better fit |
| How sensitive are you to bodily tension, appetite change, or sleep disruption? | This affects both the starting medication and the pace of titration |
| What co-occurring conditions are present? | Autism, anxiety, low mood, burnout, and sleep problems can shift the balance significantly |
This is why specialist prescribing in adult ADHD can look more nuanced than online comparisons suggest. The decision is less about picking a winner between two stimulant names, and more about matching a medication profile to the person sitting in front of you.
Your Assessment and Titration Journey with Us
Starting treatment is easier when the process is clear. The usual route begins with a thorough psychiatric assessment to confirm that ADHD is the right diagnosis, consider overlapping conditions, and decide whether medication is appropriate.
If medication is offered, titration follows. That means starting at a low dose, reviewing carefully, and adjusting in stages until benefits are clear and side effects are acceptable. Good titration is not rushed. It relies on feedback about concentration, motivation, emotional steadiness, sleep, appetite, and the overall feel of the medication through a normal week.
For adults with co-occurring autism or complex mental health histories, that structured supervision matters even more. It allows treatment to be adjusted with care, rather than leaving you to interpret every change on your own. A proper process doesn't just aim for symptom relief. It aims for a treatment plan that is safe, sustainable, and realistic in day-to-day life.
If you're considering ADHD assessment or medication support, Insight Diagnostics Global offers consultant-led care for adults, including ADHD and autism assessments, titration, and follow-up monitoring in a structured UK clinical model.