

When families first hear about OCD and alcoholism, they often assume these are separate problems that happened to collide. Clinically, that's often not what we see. In the UK, people with OCD have a 4.5-fold increased risk of developing an alcohol-related disorder, and by age 32 the cumulative incidence of alcohol and drug-related disorders in people with OCD reaches 23%, compared with 5% in the general population (UKAT on OCD and addiction).
That changes the conversation. It means drinking in someone with OCD isn't always a side issue. Sometimes it becomes part of the illness pattern itself, especially when alcohol is being used to dampen intrusive thoughts, physical tension, shame, or social discomfort. If ADHD, autism, anxiety, depression, or long delays in assessment are also in the background, the picture can become harder to recognise.
Leading with extensive experience, top, leading Consultant Psychiatrists in neurodevelopmental and personality disorder work, including Dr Sai Achuthan, services focused on Autism and ADHD and mental health along side psychological assessment have helped shape a more joined-up way of thinking about complex presentations in the UK. For readers trying to make sense of overlapping symptoms, it can also help to understand how anxiety is assessed more broadly in UK practice, including this overview of an anxiety diagnosis in the UK.
If you're trying to understand a partner, adult child, friend, or yourself, it also helps to see the broader impact of mental health on addiction. That wider lens matters, because alcohol misuse rarely develops in a psychological vacuum.
The Reality of OCD and Alcoholism
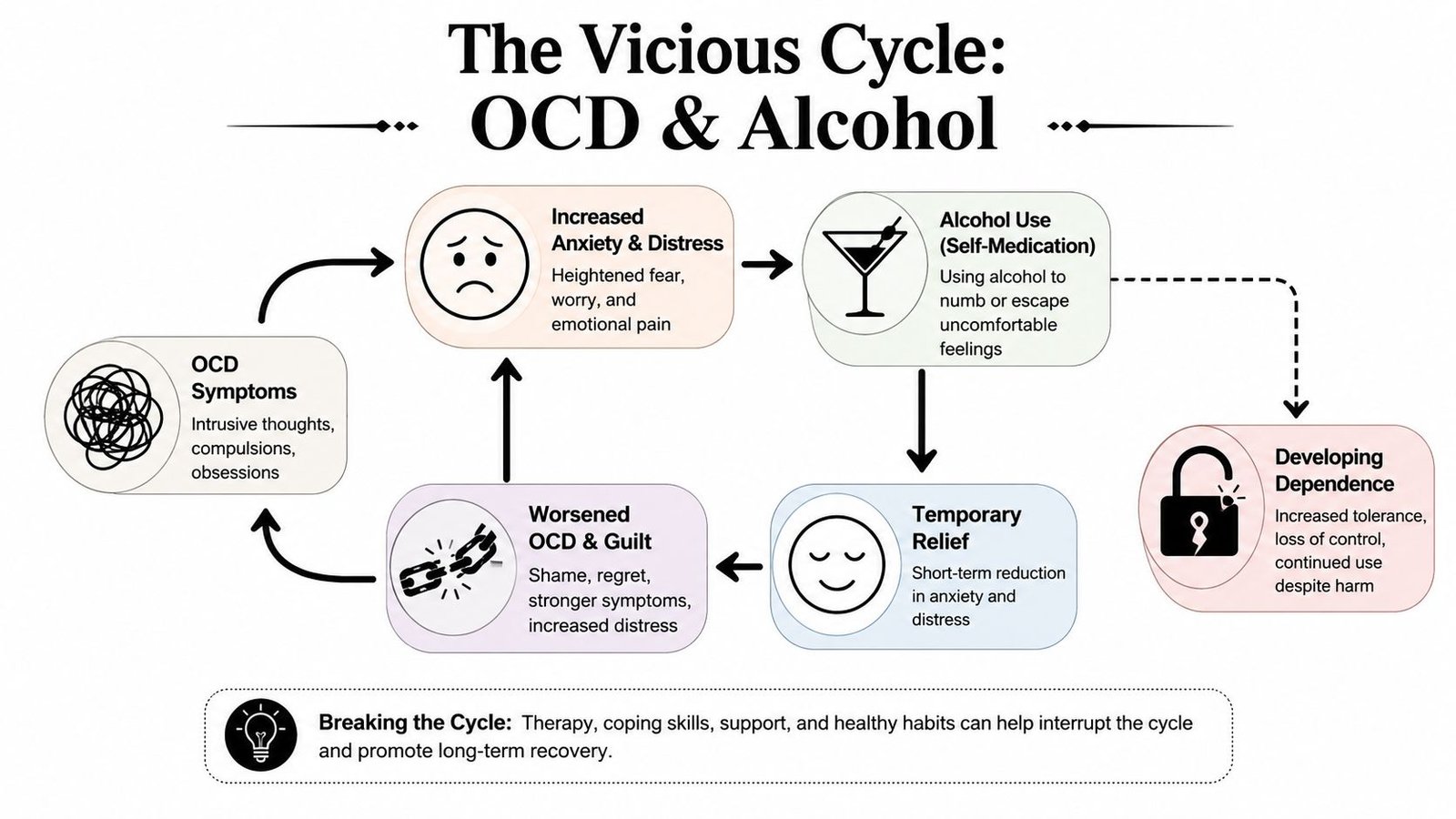
The most important starting point is this. OCD is not a personality quirk, and alcohol misuse is not just “bad coping”. Both are serious conditions, and when they occur together they can lock a person into a very punishing cycle.
A person may drink because their mind won't stop. They may feel trapped by contamination fears, checking rituals, intrusive sexual or violent thoughts, or relentless doubt. Alcohol can seem to offer a short period of quiet. For a few hours, the edge comes off.
Then the second half of the cycle arrives. Sleep becomes poorer. Anxiety rebounds. Shame grows. Concentration drops. Obsessions can feel louder, not softer. That often leads to more drinking, more secrecy, and more confusion about what is causing what.
Why families often miss it
Families usually recognise one side before the other.
Some notice the rituals, reassurance-seeking, or avoidance but don't realise alcohol has become part of the coping system. Others notice the drinking and assume the obsessive symptoms are “just stress”. In practice, both may be active at the same time.
Clinical reality: when OCD and alcohol problems coexist, treating only the visible part often leaves the hidden driver untouched.
This is one reason people can spend a long time in services without feeling fully understood. If the assessment focuses only on substance use, the OCD may be underexplained. If it focuses only on OCD, the role of alcohol in maintaining distress may be minimised.
A more hopeful way to frame it
The good news is that this pattern is recognised. It's not unusual, it's not a moral failing, and it's not beyond treatment. The key is to stop asking, “Which problem came first?” and start asking, “How are these problems interacting right now?”
That shift opens the door to better assessment, clearer diagnosis, and treatment that fits the person in front of you.
Understanding the Vicious Cycle
One of the clearest ways to understand OCD and alcoholism is through the idea of self-medication. That phrase can sound too simple, so let's make it more practical. A person with OCD may not drink for pleasure in the way others imagine. They may drink to slow down a mind that feels unbearable.
What self-medication can look like
For one person, it might mean drinking before bed because intrusive thoughts become louder at night.
For another, it might mean having alcohol before social situations because obsessions and self-monitoring become intolerable around other people.
For someone else, it may start as “just taking the edge off” after rituals, panic, or mental exhaustion. The intention is relief, not intoxication. But the brain still learns that alcohol is a fast route away from distress.
Why the relief doesn't last
Alcohol may reduce tension in the moment, but it doesn't resolve the obsessional process. The intrusive thought returns. The urge to neutralise it returns. Often the person then has two problems instead of one. The original OCD remains, and now there is alcohol-related craving, guilt, disrupted sleep, and loss of confidence.
That's part of why people often say they feel worse the next day even if the drinking initially “worked”.
A useful way to distinguish OCD from casual stress is to ask what happens after temporary relief. In OCD, reassurance and rituals usually need repeating. With alcohol in the picture, the same repetition can happen through drinking.
The amplifiers of risk
This link becomes stronger when other emotional vulnerabilities are present. The relationship between unhealthy alcohol use and obsessive-compulsive symptoms intensifies as physical and social anxiety sensitivity and general depression increase. That means some people aren't just managing obsessions. They're also managing fear of bodily sensations, fear of social judgement, and low mood at the same time.
Here's a simple way to think about those factors:
- Physical anxiety sensitivity means bodily symptoms such as a racing heart, dizziness, or tension feel especially alarming.
- Social anxiety sensitivity means embarrassment, scrutiny, or fear of being judged can become highly distressing.
- Depression lowers resilience and can make any quick relief feel harder to resist.
When alcohol is being used to manage obsessional anxiety, social discomfort, and low mood at once, the cycle tightens quickly.
Why this isn't about willpower
Families sometimes ask, “If they know alcohol makes things worse, why can't they stop?” The answer usually isn't lack of insight. It's that the short-term payoff is powerful enough to override the long-term cost, especially when distress is high.
That's why a moral lecture rarely helps. A proper formulation does. Clinicians need to understand what the alcohol is doing for the person, even if it's causing harm. Once that function becomes clear, treatment can start replacing alcohol with safer and more effective ways of tolerating obsessional distress.
Recognising Overlapping Symptoms
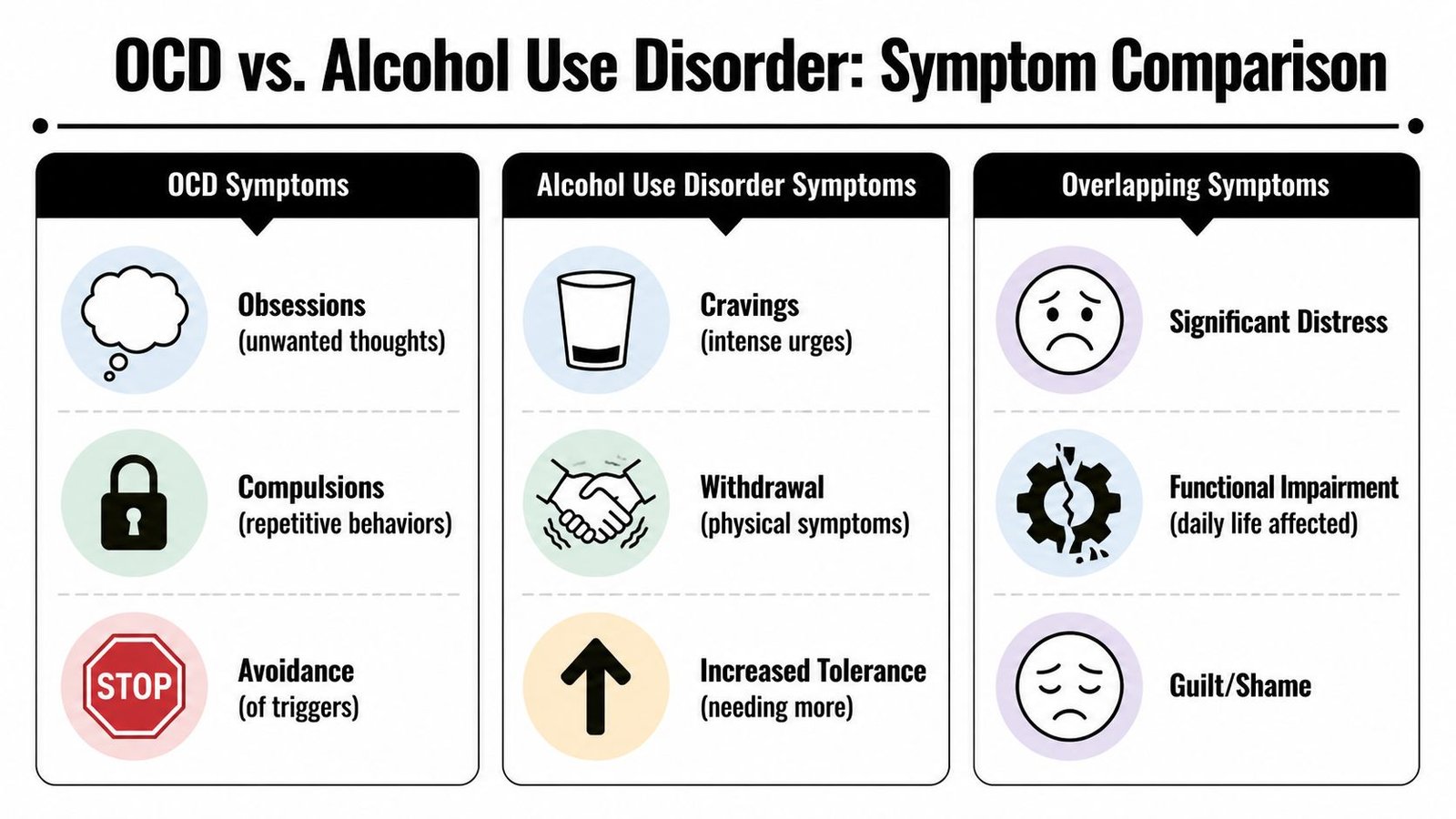
People get confused about symptoms for good reason. OCD and alcohol problems can look similar on the surface, even when the inner experience is different. A repeated behaviour doesn't always mean the same thing.
The key question is motivation
The same action can come from very different mental states.
If someone repeatedly checks whether they've locked the door because they feel a catastrophic fear they might harm others through negligence, that points towards OCD.
If someone repeatedly thinks about when they can next drink, hides alcohol, and feels driven by craving or withdrawal relief, that points more towards alcohol dependence.
Sometimes both are present. That's where the picture becomes muddy.
A simple comparison
| Behaviour | More suggestive of OCD | More suggestive of alcohol misuse |
|---|---|---|
| Repetition | Done to reduce fear or prevent imagined harm | Done to obtain alcohol, relieve craving, or avoid withdrawal |
| Thought pattern | Intrusive, unwanted, ego-dystonic thoughts | Preoccupation with drinking, access, timing, concealment |
| Emotional aftermath | Brief relief, then doubt returns | Brief relief, then guilt, craving, or physical consequences |
| Trigger | Obsession, uncertainty, disgust, fear | Stress, cue exposure, habit, social setting, withdrawal |
Examples that often confuse people
A person pours a drink every evening in exactly the same glass, at the same time, with a strict sequence. Is that a compulsion or dependence? The answer depends on what happens internally if the pattern is interrupted.
If the distress centres on “something terrible will happen unless I do this correctly”, that sounds more obsessional. If the distress centres on “I need this drink now or I can't settle”, dependence may be more central. If both thoughts are present, clinicians need to assess both.
Another example is reassurance-seeking. Someone with OCD may repeatedly ask, “Am I a bad person?” Someone with alcohol dependence may repeatedly seek reassurance that their drinking “isn't that bad”. Both involve distress and shame. The drivers differ.
A practical rule: don't focus only on the behaviour. Ask what fear, urge, or expectation sits underneath it.
When alcohol creates a second layer of obsession
Longer-term alcohol misuse can create persistent mental preoccupation with drinking. That can feel obsessive, but it isn't always OCD in the formal sense. A person may spend hours planning when they can drink, worrying about supply, promising themselves they'll stop, then returning to the same mental loop.
This doesn't mean the original OCD has disappeared. It means the person may now be carrying two separate streams of repetitive distress. One is obsessional. The other is addiction-related.
What helps at assessment
If you're preparing for an appointment, it often helps to note:
What happens just before the behaviour
Is there an intrusive thought, a wave of anxiety, a physical panic sensation, a craving, or a low mood?What the person hopes the action will achieve
Prevent harm, gain certainty, calm the body, feel numb, or get through social contact?How long relief lasts
Minutes, hours, or not at all?
That sort of detail gives a clinician something much more useful than a label like “compulsive”.
The Impact on Neurodevelopmental Conditions
When ADHD or autism are part of the picture, OCD and alcoholism can become harder to spot and harder to untangle. The reason isn't that these conditions are the same. They aren't. The reason is that they can affect emotional regulation, sensory tolerance, attention, impulsivity, and coping style in ways that complicate the presentation.
ADHD, impulsivity, and fast relief
An adult with ADHD may already struggle with frustration, restlessness, inconsistency, and acting quickly under emotional strain. If that person also has OCD, alcohol can become an accessible form of short-term relief. It may not be chosen after careful thought. It may be chosen because distress is high and the barrier to acting on an urge is lower.
In clinical work, this matters because the person may describe “chaos”, “burnout”, or “always messing things up” before they ever mention obsessional thinking.
Autism, sensory strain, and social exhaustion
For autistic adults, the pressure can look different. Some feel overwhelmed by sensory input, rigid routines being disrupted, or the demands of masking in social environments. If obsessional fears or ritualised coping are present as well, alcohol can start to function as a blunt instrument for shutting the whole system down.
That doesn't solve the underlying mismatch. It often adds another layer of difficulty, especially around sleep, communication, and recovery after social effort.
A full mental health assessment should ask not only “What symptoms are present?” but also “What is this person trying to cope with?”
Why complete assessment is often delayed
This broader view is especially important in the UK because access delays can leave people carrying several interacting difficulties without a coherent formulation. In December 2023, the number of patients in England with an open referral for suspected autism reached 172,022, with 79% of those waiting over 13 weeks not yet receiving their first appointment (Nuffield Trust on autism and ADHD waiting lists).
For people trying to understand traits across autism, ADHD, obsessive symptoms, alcohol use, and anxiety, that delay can be costly. During long waits, coping strategies often harden into patterns. For a broader overview of how these conditions can overlap in adults, this discussion of autism and ADHD is a useful starting point.
Why the neurodiversity lens matters
Without a neurodevelopmental lens, clinicians may misread impulsivity as non-compliance, rigidity as “just anxiety”, or alcohol use as the whole story. With that lens, assessment becomes more accurate. It can explain why one person drinks after social overload, another after obsessive doubt, and another after both.
How to Get a Comprehensive Assessment
The hardest part for many adults is not deciding whether they need help. It's figuring out what kind of help makes sense when symptoms overlap. If OCD, alcohol misuse, anxiety, depression, ADHD traits, autistic traits, or burnout all seem relevant, a narrow assessment often leaves important pieces out.
What a good assessment should actually do
A proper psychiatric assessment isn't just a symptom checklist. It should build a timeline.
That means asking when intrusive thoughts began, when alcohol started being used as a coping tool, whether there were earlier signs of ADHD or autism, what happened at school or university, how relationships have been affected, and whether anxiety or depression sit underneath the whole pattern.
It should also ask about safety, sleep, work, physical health, family history, and current functioning. The aim is not to force everything into one diagnosis. The aim is to identify what is primary, what is secondary, and what now needs active treatment.
Questions worth expecting
A clinician assessing OCD and alcoholism alongside possible neurodevelopmental conditions will often explore:
Obsessions and rituals
What thoughts are intrusive? What behaviours or mental acts follow? How much time do they take?Alcohol pattern
When do you drink, why do you drink, what happens if you try not to, and what are the consequences?Developmental history
Were there longstanding attention problems, sensory sensitivities, social communication differences, or repetitive patterns earlier in life?Emotional context
Is there panic, social fear, depression, trauma, shame, or exhaustion in the background?Functioning
What's happening to work, study, relationships, self-care, finances, and sleep?
For many adults, reading a plain explanation of what a mental health assessment involves helps reduce some of the uncertainty before the first appointment.
Why joined-up triage matters
A major UK gap is that dual presentations are often not screened for together early enough. Although 23% of UK OCD patients develop alcohol-related disorders by age 32, current UK access routes, including Right to Choose pathways for ADHD and ASD, often don't consistently integrate screening for these comorbidities, leaving an important gap in triage and dual-diagnosis care.
That matters because the person may enter a pathway for one reason and still leave without a clear explanation for the rest of their symptoms.
The best assessment doesn't ask a person to choose one label. It asks which combination of conditions best explains the whole pattern.
Right to Choose and specialist routes
For adults in England, Right to Choose can be an important route when NHS waiting times are long. In practice, many people seek an ADHD or autism assessment because those traits are the most recognisable part of their difficulty. During a specialist assessment, it may become clear that obsessive-compulsive symptoms, harmful drinking, anxiety, or mood problems also need formal attention.
That's one reason consultant-led services can be helpful. Experienced psychiatrists are trained to think across diagnoses rather than inside one box. In more complex cases, that breadth matters.
A short explainer on the wider context is helpful here:
What to prepare before the appointment
You don't need a perfect summary. But it helps to bring:
A symptom timeline
Rough notes on when obsessions, rituals, drinking, panic, low mood, or attention problems became noticeable.Examples from daily life
Not just “I get anxious”, but “I spend an hour checking appliances” or “I drink before social events because my thoughts escalate”.Collateral information if available
School reports, partner observations, or family descriptions can be useful, especially when ADHD or autism are being considered.
The clearer the story, the easier it is for a psychiatrist to identify the right next step.
Integrated Treatment and Recovery Pathways
When OCD and alcoholism occur together, separate treatment tracks often miss the point. If a service tries to reduce drinking without addressing obsessional anxiety, alcohol may remain the person's fastest coping tool. If a service treats OCD without addressing alcohol dependence, therapy may be undermined by intoxication, withdrawal, avoidance, and unstable routines.
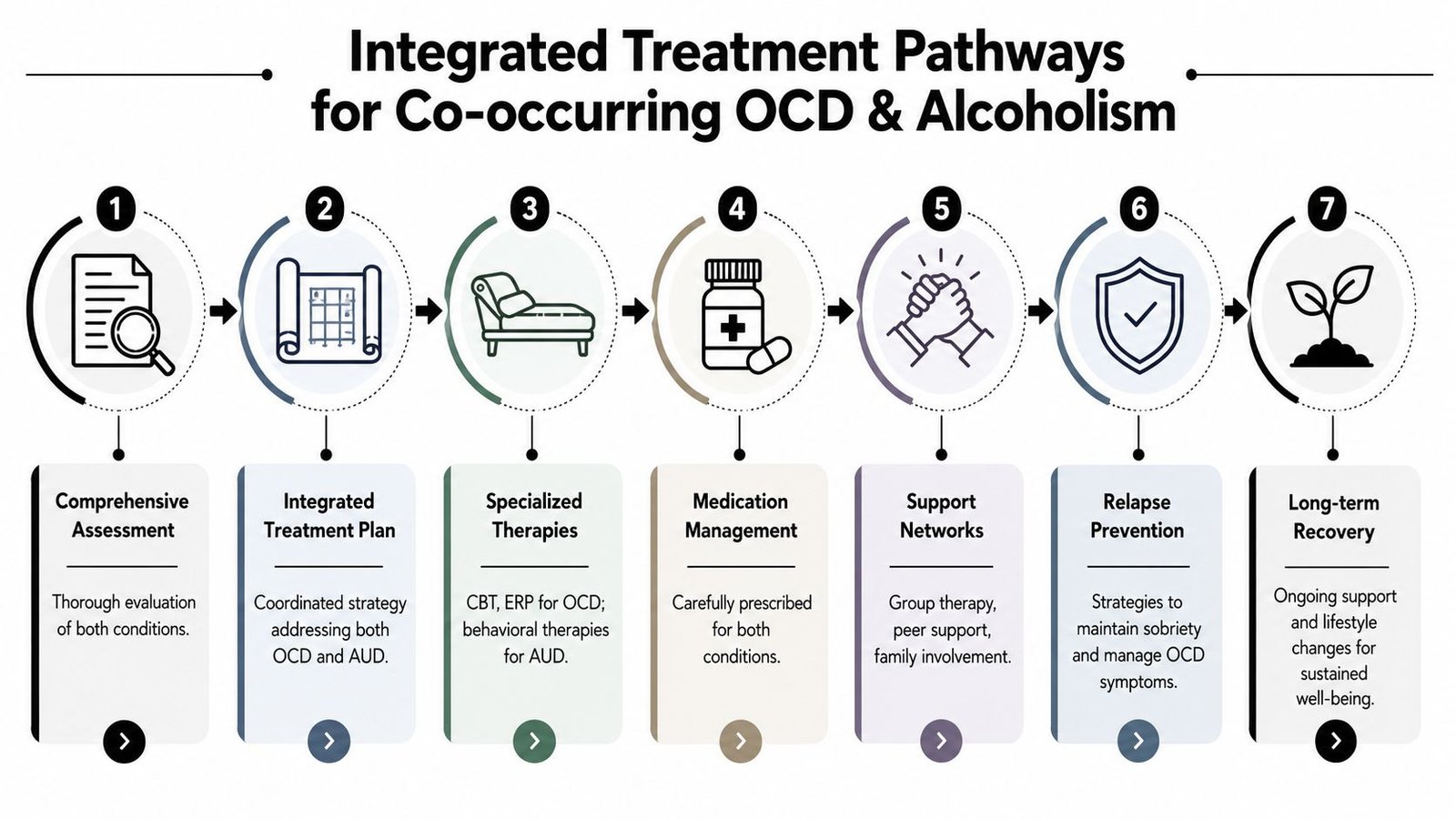
Research supports an integrated approach. Treatment that combines Cognitive Behavioural Therapy (CBT), including Exposure and Response Prevention (ERP), with structured detoxification has been shown to increase 12-month abstinence rates and reduce OCD symptom severity more effectively than sequential or single-disorder treatment (PMC review on co-occurring OCD and alcohol use disorder).
Why integrated care works better
ERP is the best-known psychological treatment for OCD. It helps a person face feared thoughts, situations, or sensations without performing the usual compulsion. That's powerful, but it's hard to do if alcohol is being used at the same time to escape distress.
Structured alcohol treatment helps stabilise the system. It creates a more reliable platform for therapy, sleep, and emotional regulation.
Combined treatment also prevents a common problem. The person stops drinking, feels a surge of obsessional anxiety, and then relapses because nobody prepared them for that rebound.
What treatment may include
Different people need different combinations, but a thoughtful plan often covers the following:
Psychological therapy for OCD
ERP is usually central. The work is gradual and planned. It isn't about forcing distress for its own sake.Alcohol-focused intervention
This may involve medically supervised detoxification where appropriate, relapse-prevention work, behavioural strategies, and regular monitoring.Medication review
OCD medications, including SSRIs where clinically indicated, need to be considered in the context of alcohol use, adherence, side effects, and safety.Mood and anxiety treatment
Depression and anxiety sensitivity often maintain the cycle, so they shouldn't be treated as background noise.
What recovery often looks like in real life
Recovery is rarely a neat straight line. One week may be about reducing ritualised reassurance. Another may be about getting through evenings without drinking. Another may be about attending a social event without alcohol and without compulsive checking afterwards.
A skilled team helps the person build tolerance for uncertainty and discomfort without falling back on the old solution.
Recovery usually begins when the person no longer has to choose between “treat my OCD” and “treat my drinking”. Both are treated as part of one formulation.
The role of family and support systems
Families can help, but they often need guidance. Reassurance can accidentally feed OCD. Monitoring can accidentally become conflict. Pleading with someone to “just stop” can increase secrecy if alcohol is serving a powerful emotional function.
Helpful family involvement usually includes:
Learning the pattern
Understanding when reassurance, accommodation, or criticism are keeping the cycle alive.Supporting treatment goals
Encouraging attendance, medication adherence where prescribed, and agreed plans around triggers.Reducing shame
Shame makes both OCD and alcohol problems harder to disclose. A calmer, more boundaried response usually works better.
A balanced expectation
Integrated treatment is demanding, but it's realistic. People do improve. What tends to help most is accurate diagnosis, safe management of alcohol problems, evidence-based OCD treatment, and a plan that also accounts for ADHD, autism, or mood difficulties when those are present.
Coping Strategies and Finding UK Support
Treatment is essential when symptoms are entrenched, but day-to-day coping also matters. The aim isn't to “white-knuckle” your way through OCD and alcoholism. The aim is to reduce the need for alcohol as an emotional tool.
Coping strategies that can help
Delay the first response
If you feel the urge to drink or perform a ritual, try building a short pause first. Even a brief delay can help you notice whether the driver is fear, craving, exhaustion, or social overload.Name the trigger precisely
“I feel bad” is too broad to work with. “I'm having contamination obsessions after work” or “I'm dreading a social event and want alcohol to numb it” gives you something concrete.Use structured evenings
Many people drink when unstructured time meets obsessive rumination. A written evening plan can reduce drift and cut exposure to high-risk moments.Practise graded exposure with support
If your team has recommended ERP-style work, start with manageable targets. Don't improvise intense exposure alone when alcohol use is unstable.Reduce secrecy
Hidden routines feed both conditions. Telling one trusted person what's happening often lowers the pressure.Protect sleep
Tired brains are more obsession-prone and less able to resist urges. Sleep won't cure either condition, but poor sleep often worsens both.
UK support options worth knowing
In the UK, many people benefit from combining formal treatment with charities, peer groups, and practical information. OCD-UK, Alcohol Change UK, and mutual-aid groups such as AA can all form part of a support network, depending on the person's needs and preferences.
For adults seeking broader psychiatric clarification around overlapping conditions, there are also specialist mental health pathways focused on mental health services for adults. If you're reading from outside the UK or comparing models of care, some people also look at examples of California dual diagnosis treatment programs to understand how integrated services are structured elsewhere.
If alcohol has become unsafe to stop suddenly, seek medical advice urgently. Withdrawal can require supervised care.
When to seek urgent help
Assessment and planned treatment are appropriate for many people. Emergencies are different.
If someone is at immediate risk, severely intoxicated, suicidal, confused, hallucinating, or medically unwell, use urgent services. In the UK, contact NHS 111 for urgent support or call 999 in an emergency. Specialist assessment services are not crisis services.
Recovery starts with recognising the pattern clearly. Once OCD and alcohol use are understood together, the path forward usually becomes much more practical.
If you want a consultant-led, adult mental health assessment that considers ADHD, autism, OCD, anxiety, depression, and overlapping presentations in one structured pathway, Insight Diagnostics Global offers online and face-to-face assessments for adults aged 18 and over. The service is CQC-regulated, led by psychiatrists on the GMC Specialist Register, and designed to provide clear triage, detailed reports, and personalised recommendations. It isn't a crisis service, so for urgent risk contact NHS 111 or call 999.