

You wake at 4am with your chest tight, your mind already running through work, family, money, health, and the possibility that you've somehow missed something important. By breakfast, you're functioning on the outside and exhausted underneath. You may have tried to reassure yourself that it's “just stress”, yet the same pattern keeps returning.
For many adults, that's the moment the search for an anxiety diagnosis in the UK begins. Not because they want a label, but because they want an explanation that makes sense. They want to know why their body won't settle, why ordinary decisions feel loaded, and why coping strategies that help other people don't seem to touch the core problem.
That question becomes even more important when anxiety sits alongside traits of ADHD, autism, burnout, panic, or long-standing emotional overwhelm. In clinic, that overlap is where many people get stuck. They've been told they're anxious, which may be true, but it may not be the whole picture.
Navigating Your Concerns About Anxiety
A common starting point is uncertainty. Your heart races. You overthink messages before sending them. You avoid meetings, public transport, supermarkets, or social plans because they feel too much. Then you wonder whether you're dealing with an anxiety disorder or a difficult period.
You're not alone in asking that. In March 2023, 20% of UK adults reported feeling anxious most or all of the time in the previous two weeks, and in 2023–24 there were 204,526 new referrals for patients aged 17 or under where anxiety was the primary cause, with the paper noting that this was more than double the pre-pandemic rate (UK anxiety demand data).
That doesn't mean every worried person needs a formal diagnosis. It does mean persistent anxiety is common, clinically relevant, and worth taking seriously when it starts shaping your sleep, concentration, relationships, confidence, or physical health.
When the symptom feels physical
Many adults first present with the body rather than the emotion. They notice palpitations, dizziness, chest tightness, nausea, trembling, or a sense of impending collapse. That often leads to a frightening thought: “What if this isn't anxiety at all?”
If that sounds familiar, a practical explanation of why anxiety can affect the heart and chest sensations can help you separate a common anxiety pattern from a medical emergency, though new or severe symptoms should still be medically checked.
Anxiety often becomes most convincing when it borrows the language of physical illness.
When coping advice doesn't match the problem
Generic advice can miss the mark. Someone with mild situational nerves may benefit from gradual exposure. Someone with panic, autistic sensory overload, or untreated ADHD may need a far more individualized plan. Even everyday examples matter. If exercise spaces trigger self-consciousness or overstimulation, practical guidance on how to overcome gym anxiety can be useful, but only if the anxiety itself has been understood properly first.
A good assessment doesn't dismiss your distress. It sorts out what kind of anxiety you're dealing with, what else may be sitting underneath it, and what the next step should be.
What an Anxiety Diagnosis Really Means
An anxiety diagnosis isn't a judgement on your personality. It's a clinical formulation of a pattern. A clinician looks at the type of symptoms, how long they've been present, how intense they are, and what they're doing to your day-to-day functioning.
In UK practice, clinicians may use frameworks from DSM-5 or ICD-11, but the practical questions are simpler than the manuals suggest. Is this worry persistent rather than occasional? Is it excessive relative to the situation? Does it interfere with work, study, sleep, relationships, or self-care? Are there panic symptoms, avoidance, obsessive features, trauma symptoms, low mood, or neurodevelopmental traits mixed in?
Everyday anxiety versus disorder level anxiety
Everyone experiences anxiety. A diagnosis comes into focus when the anxiety is persistent, impairing, and structured in a recognisable clinical pattern.
For example, with generalised anxiety disorder, NHS guidance typically expects symptoms to have been present for at least six months and to be affecting daily life. That's different from having a stressful fortnight during exams, after a breakup, or in the middle of a demanding project.
A helpful way to think about it is as a symptom cluster:
- Worry: hard to control, present across several areas of life
- Body symptoms: tension, restlessness, poor sleep, fatigue
- Cognitive effects: poor concentration, indecision, anticipatory dread
- Functional impact: reduced confidence, avoidance, impaired performance
Why the label can help
A diagnosis can clarify treatment options, workplace adjustments, referral routes, and the difference between “coping badly” and “having a treatable condition”. It can also stop the endless self-blame that many anxious adults carry.
National figures show why this matters. Generalised anxiety disorder is estimated to affect up to 8 in 100 people in any given week in England, and 1 in 5 adults (20.2%) in England were living with a common mental health problem, with a higher burden in women at 24.2% compared with 15.4% in men (Mind's mental health facts and statistics).
A diagnosis should create clarity. If it leaves you more confused than before, the assessment probably wasn't deep enough.
Who Can Provide an Anxiety Diagnosis in the UK
Individuals often begin with a GP, and that makes sense. A GP can rule out common physical contributors, ask about risk, review medication or substance use, begin initial treatment, and decide whether you need referral to talking therapies, community mental health support, or a specialist assessment.

GPs are often the right first step. They are not always the final step. That matters particularly when anxiety is chronic, treatment-resistant, mixed with depression, complicated by trauma, or possibly linked with autism or ADHD.
Why GP records can look vague
Primary care coding is often broad rather than highly specific. A large UK primary care analysis found that ‘anxiety states', ‘anxiety with depression', and ‘panic attack' made up 82.6% of diagnosis episodes, while formal codes like GAD represented under 2% (UK primary care coding study).
That doesn't mean your GP has done something wrong. It usually means general practice is capturing the immediate clinical picture, often before disorder subtyping has been worked through in depth.
The different roles
| Professional | What they usually do | Key limitation or strength |
|---|---|---|
| GP | First assessment, medical screening, initial treatment, referral | Good for triage. Limited time for complex diagnostic untangling |
| Clinical psychologist | Detailed psychological assessment and therapy formulation | Usually doesn't prescribe medication |
| Consultant psychiatrist | Diagnostic assessment, differential diagnosis, medication advice and prescribing | Particularly useful where symptoms overlap across conditions |
For adults with a more layered presentation, a Consultant Psychiatrist is often the most useful assessor because they can weigh mental health diagnoses against neurodevelopmental conditions, personality factors, trauma history, sleep disruption, substance effects, and physical contributors.
A clinician with experience in neurodevelopmental presentations, including consultants such as Dr Sai Achuthan, may be especially relevant when anxiety could be secondary to lifelong attention difficulties, sensory overwhelm, masking, or social communication strain.
A short overview of mental health assessment can also help before you book:
If the question in your mind is “why does none of this fit neatly?”, that's usually a sign to seek specialist assessment rather than another brief review.
NHS vs Private Diagnostic Pathways Explained
People often assume there are only two choices. Wait on the NHS or pay privately. In practice, the picture is a little more nuanced.
How the NHS route usually works
The NHS pathway often begins with a GP appointment. From there, you may be offered brief intervention, medication, a referral for talking therapy, or onward referral if the presentation looks more complex.
This route can work well when symptoms are relatively straightforward and risk is low. It can be less satisfactory when the primary question is diagnostic complexity rather than symptom relief alone. That includes adults who suspect ADHD, autism, panic disorder, obsessive features, trauma-related anxiety, or burnout layered on top of longstanding coping difficulties.
In England, some patients also explore Right to Choose, which can allow NHS-funded assessment with an eligible independent provider. The administrative details depend on service type, local referral practice, and whether the provider accepts that route for the assessment in question.
How the private route differs
Private assessment is usually chosen for speed, clinician choice, and depth. Some adults self-fund because they want an answer sooner. Others use private medical insurance, where cover depends on policy terms and pre-authorisation.
A private route can be particularly useful when you need:
- Diagnostic precision: not just “anxiety”, but whether it is GAD, panic, social anxiety, health anxiety, or anxiety linked to ADHD or autism
- Flexible appointments: useful for professionals, students, carers, and people who find standard clinic settings difficult
- Clear documentation: a written report for treatment planning, work, study support, or ongoing care
One option adults consider is a general mental health assessment near them or online, especially when they want a broader psychiatric view rather than a narrow symptom checklist.
Side by side comparison
| Factor | NHS Pathway | Private Pathway |
|---|---|---|
| How you start | Usually via GP | Self-referral, GP suggestion, or insurer authorisation |
| Pace | Depends on local service capacity and referral thresholds | Usually more flexible and faster to arrange |
| Choice of clinician | Limited by local service structure | Greater choice of specialist background |
| Assessment scope | Often focused on current symptoms and immediate treatment needs | Often broader, especially for overlap with ADHD, autism, trauma, or mood symptoms |
| Medication | GP or NHS psychiatry depending on pathway | Depends on assessor type and follow-up arrangements |
| Cost | NHS funded | Self-funded or insurance-based |
| Best suited to | Straightforward initial presentations | Complex, overlapping, or time-sensitive presentations |
The trade-off is straightforward. NHS care is essential and often the right place to begin. Private care can be useful when the issue isn't just access to treatment, but access to the right formulation.
The Critical Overlap of Anxiety ADHD and Autism
A common diagnostic challenge for many adults is that they get misread. They present with anxiety, and anxiety is certainly present, but it may be secondary, intertwined, or partly the result of years spent coping with an unidentified neurodevelopmental profile.
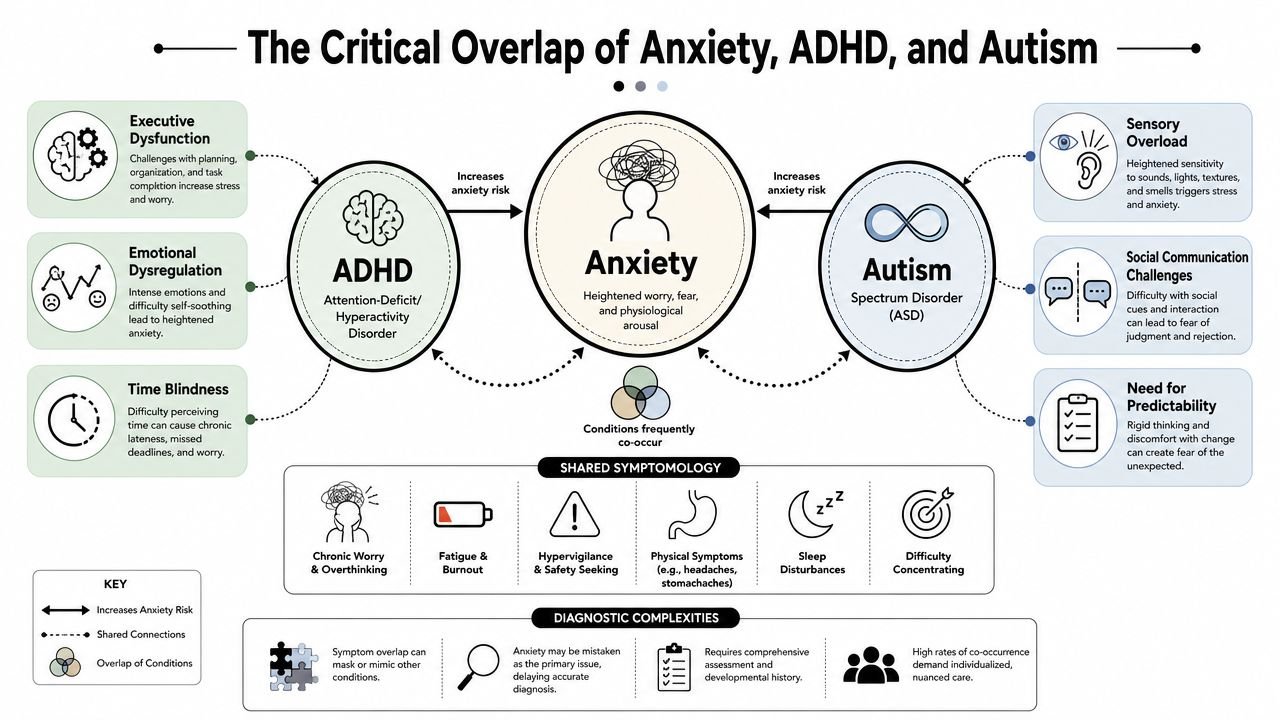
How ADHD can look like anxiety
An adult with ADHD may look anxious because they are chronically behind, mentally overactive, emotionally reactive, and anticipating failure. They may describe dread before simple tasks, racing thoughts at bedtime, panic around deadlines, and shame after missed appointments or unfinished work.
From the outside, that can be coded as anxiety alone. Sometimes it is anxiety alone. Sometimes the anxiety is the understandable consequence of unmanaged ADHD.
Clues that push the assessment further include:
- Lifelong disorganisation: not just recent stress
- Task paralysis: especially for boring, multi-step, or administratively heavy tasks
- Emotional swings: rapid frustration, overwhelm, or rejection sensitivity
- Variable performance: capable one day, stuck the next
How autism can look like anxiety
Autistic adults often describe chronic anxiety around uncertainty, sensory overload, social ambiguity, masking, and change. A crowded office, a noisy café, or an unstructured social event can trigger genuine distress. That distress may then be labelled social anxiety, general anxiety, or agoraphobia without anyone examining the underlying autistic pattern.
A few practical distinctions matter:
| Presentation | Could be anxiety | Could be autism-related |
|---|---|---|
| Avoids social events | Fear of judgement or embarrassment | Sensory overload, social fatigue, difficulty reading group dynamics |
| Needs routine | Worry if plans change | Strong preference for predictability and cognitive stability |
| Shuts down under pressure | Panic or overwhelm | Overload response linked to processing demands |
Why comprehensive assessment matters
A narrow anxiety assessment may ask, “How worried are you?” A better assessment also asks, “What has your mind been doing since childhood, how do you process people and environments, and what happens when demands exceed capacity?”
That difference changes treatment. Standard CBT can help many people, but it may need adaptation if the person is autistic. Anxiety management also won't solve executive dysfunction if ADHD is central to the picture.
For some adults, support outside formal healthcare also matters. If social connection feels difficult in conventional dating spaces, a specialist community such as an autism dating site may offer a more accessible way to build relationships without the same degree of masking pressure.
If you're also wondering whether anxiety runs in families or clusters with broader developmental patterns, this discussion of whether anxiety disorders can have a genetic component is a useful companion.
The most common diagnostic error isn't inventing anxiety where none exists. It's stopping at anxiety when the story is wider.
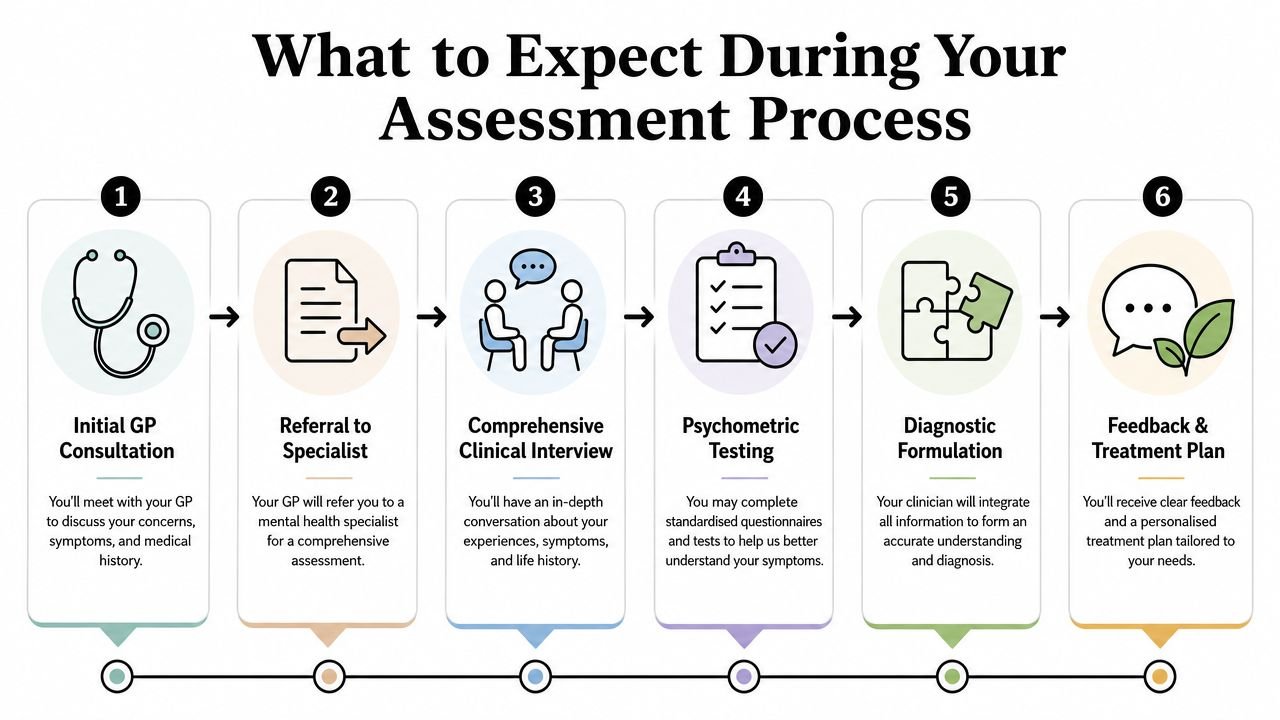
What to Expect During Your Assessment Process
Many adults are more frightened of the assessment than of the diagnosis itself. They worry they'll say it wrong, forget important details, or be judged as overreacting. A competent assessment shouldn't feel like an interrogation. It should feel organised, collaborative, and clinically curious.
The usual stages
A modern assessment often includes most of the following steps, though the exact order varies by service.
Initial triage
This checks whether the service is appropriate, whether you need a psychiatric or psychological assessment, and whether there are urgent risks that need a different route.Questionnaires
Standardised tools can help structure the picture. They don't diagnose you on their own, but they can highlight severity, patterns, and associated symptoms.Clinical interview
This is the core part. The clinician asks about your current symptoms, onset, triggers, functioning, background history, relationships, education, work, sleep, physical health, and any previous treatment.Differential diagnosis
Expertise is paramount. The clinician weighs anxiety against panic disorder, depression, OCD, trauma-related conditions, ADHD, autism, substance effects, and medical explanations.Formulation and feedback
Good feedback joins the dots. It explains not only what diagnosis fits, but why.
What helps you prepare
You don't need to arrive with perfect notes, but a few points can make the appointment more useful:
- Timeline: when symptoms started, and whether they came on suddenly or built up gradually
- Patterns: what reliably triggers the anxiety, and what makes it worse
- Impact: examples from work, relationships, sleep, driving, study, or daily tasks
- History: previous counselling, CBT, antidepressants, ADHD concerns, autistic traits, panic attacks, burnout, or trauma
A fuller explanation of what happens in a psychiatric assessment can reduce a lot of anticipatory fear before the appointment itself.
What a consultant-led process should include
For adults wanting a broad psychiatric view, some services offer structured assessments with triage, interview, formal report, and follow-up options. Insight Diagnostics Global is one such consultant-led service for adults, offering online and face-to-face mental health assessments, with psychiatrists on the GMC Specialist Register and CQC regulation as part of its service framework.
The key point isn't the brand. It's the structure. You want a process that is careful enough to identify what fits, what doesn't, and what needs adaptation because of neurodiversity or comorbidity.
Bring examples, not polished explanations. “I rehearse phone calls for twenty minutes” is often more clinically useful than “I get anxious sometimes”.
Your Diagnostic Report and Treatment Options
A strong diagnostic report should do more than state a label. It should translate assessment into action.
At minimum, the report should identify the diagnosis or diagnoses considered, explain the clinical reasoning, and set out practical recommendations. If the picture is mixed, it should also say so clearly. “Anxiety symptoms present, but further assessment of ADHD traits advised” is far more useful than a vague reassurance that leaves you back where you started.
What you should expect to see
Most good reports include:
- Diagnostic conclusion: what condition best fits the presentation, and what has been ruled out
- Formulation: how symptoms developed and what maintains them
- Risk overview: any urgent concerns that need attention
- Treatment recommendations: therapy, medication review, lifestyle changes, workplace or study adjustments, or referral onward
Treatment usually works best when it matches the pattern
For some adults, CBT is the right starting point. For others, medication such as an SSRI may be discussed. If ADHD is part of the picture, treatment may need to include ADHD-specific review rather than intensifying anxiety treatment in isolation. If autism is relevant, therapy often works better when it respects sensory load, processing style, and the cost of masking.
Medication discussions need to be grounded and specific. If you're trying to understand the clinical and prescribing context around benzodiazepines, this guide to understanding Valium prescription options is a useful overview of why these medicines are treated cautiously rather than casually.
A report is most valuable when it becomes a working document. You should be able to take it to your GP, therapist, employer, university, or follow-up clinician and use it to make sensible next decisions.
Frequently Asked Questions About Anxiety Diagnosis
A diagnosis doesn't always arrive in a single neat sentence. Sometimes the first useful answer is that anxiety is present, but further assessment is needed to understand whether it is primary or part of a broader pattern.
| Question | Answer |
|---|---|
| Can a GP diagnose anxiety? | Yes. A GP can diagnose anxiety, start treatment, and refer onward. If the presentation is complex, a specialist assessment may still be needed. |
| Does it matter if my record says symptoms rather than disorder? | It can. Symptom coding is common, but if you need diagnostic clarity for treatment planning, work, study support, or overlap with ADHD or autism, a fuller assessment helps. |
| Should I choose NHS or private? | It depends on urgency, complexity, and your budget or insurance position. NHS is often the right place to start. Private can be useful if the main need is speed or diagnostic depth. |
| What if I think I have anxiety and ADHD or autism? | Say that directly at booking stage. It changes what kind of assessment is appropriate. |
| What if I'm in crisis? | Diagnostic services are not emergency services. If you feel at immediate risk, call 999. For urgent mental health support, contact NHS 111. |
If you want a structured adult mental health assessment that considers anxiety alongside ADHD, autism, mood, panic, and functional impact, Insight Diagnostics Global provides consultant-led evaluations online and face to face for adults aged 18 and over. The service is not for emergencies, but it can help when you need a clear diagnostic opinion, a written report, and practical next-step recommendations.