

A lot of adults arrive at this question sideways. They don't start by asking about genetics. They start by saying they've always been “on edge”, they lose focus under pressure, social situations feel draining, and now their child seems to show some of the same patterns. Then the family history starts to line up. An anxious parent. A sibling with ADHD traits. A grandparent who avoided people, routines, or change.
That's usually the moment the question sharpens. Is this anxiety? Is it ADHD? Is it autism? And does it run in families?
In specialist psychiatric work, that combination is common. Anxiety rarely sits in a neat box on its own. It often overlaps with neurodevelopmental differences, especially ADHD and autism, and that overlap can make self-diagnosis misleading. The useful question isn't “Which single label explains everything?” It's “What pattern has been present across development, and what is driving the current distress?”
Why Anxiety and Neurodevelopment Seem to Run in Families
A familiar story goes like this. An adult books an ADHD assessment because work has become unmanageable. They miss deadlines, feel mentally noisy, and can't switch off at night. During the assessment conversation, they describe a much longer history. Worry as a child. Social exhaustion as a teenager. Panic before ordinary tasks. Sensory discomfort they've always tried to hide.
Then they mention family members.
A parent who was “highly strung”. A brother who was always restless and impulsive. A daughter who's bright but overwhelmed by school, change, or friendships. None of that proves a diagnosis, but it does tell me something important. These patterns often cluster within families, even when the labels differ across generations.
Family patterns rarely arrive as one tidy diagnosis
In real life, family mental health histories are messy. One relative may have clear panic symptoms. Another may never have been diagnosed with anything, but has always needed strict routines, avoided social situations, or struggled with attention and emotional regulation. A third may have coped well professionally while quietly living with relentless internal anxiety.
That's one reason broad, structured assessment matters. If you're exploring overlapping traits in yourself or someone close to you, a specialist overview of autism and ADHD in adults can help frame what often gets mistaken for “just anxiety” or “just personality”.
Families don't pass down neat labels. They pass down vulnerabilities, temperaments, coping styles, and sometimes similar ways of processing the world.
Why this matters to a concerned adult
If you've noticed the same themes across generations, your instinct isn't irrational. It's often clinically useful. The mistake is jumping from “this runs in my family” to “this must be genetic and fixed”. That leap creates either fatalism or false certainty, and neither helps.
A better approach is to treat family history as one strand of evidence. It can support an assessment, sharpen the questions, and help explain why anxiety and neurodevelopmental traits so often travel together. It can't replace a proper diagnostic process.
Is Anxiety Genetic Understanding Heritability
The short answer is yes, anxiety has a genetic component. The more accurate answer is that anxiety is partly heritable, not genetically predetermined.
A useful way to think about this is to picture genes as a blueprint and life experience as the builders, weather, and materials. The blueprint matters. It influences what is more likely to be built. But it doesn't decide the final outcome on its own. Stress, relationships, trauma, physical health, sleep, neurodevelopmental profile, and life circumstances all shape how vulnerability turns into symptoms.
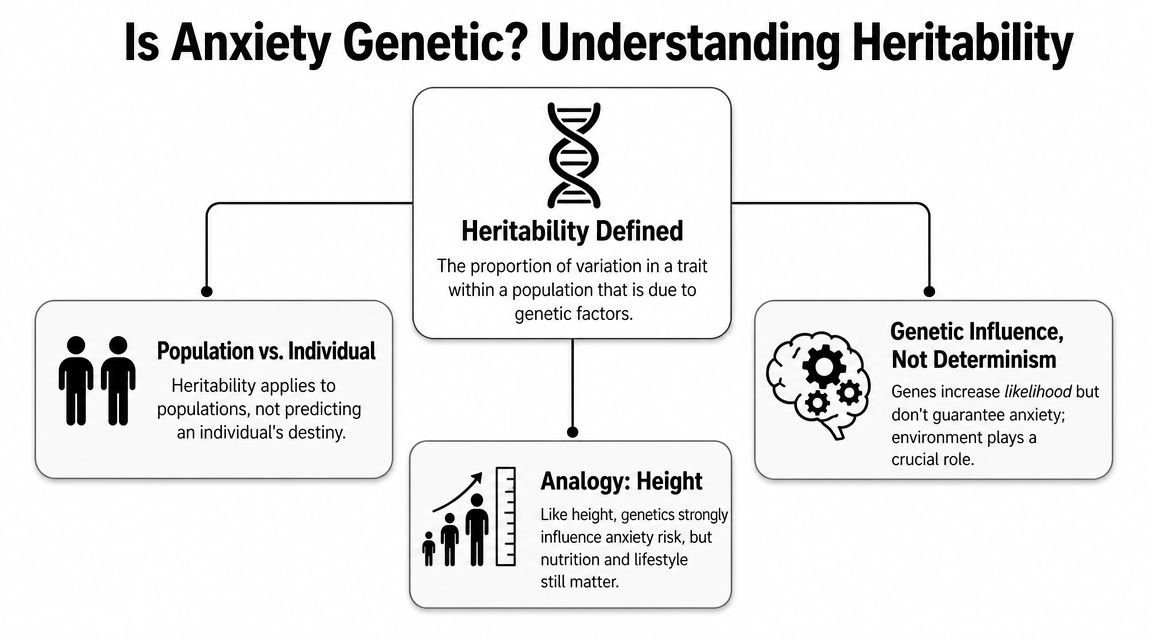
What heritability actually means
A foundational review found that anxiety disorders show moderate familial aggregation with an odds ratio of 4–6, while twin-based heritability estimates are about 30%–50% (review of anxiety genetic epidemiology). In plain English, people with affected relatives are several times more likely to have anxiety disorders than people without that family history, but genetics still explains only part of the picture.
That last part matters most. Heritability is a population concept. It does not tell you whether your anxiety is “50% genetic” as an individual. It doesn't predict destiny. It tells us that inherited factors make a meaningful contribution across groups of people.
For readers who want a practical explanation of how anxiety develops in day-to-day life, this overview of the causes of social phobia is a useful example of how biological vulnerability and lived experience interact.
A short visual explanation can help make that distinction clearer:
What this means in practice
When someone asks me whether their anxiety is genetic, I usually bring it back to three points:
- Family history matters: It's clinically relevant if close relatives have anxiety, panic, chronic worry, avoidance, ADHD traits, autistic traits, or mood problems.
- Genes are not a verdict: You can have a strong family loading and never develop a disorder. You can also develop significant anxiety without an obvious family history.
- Environment changes expression: Sleep disruption, bullying, academic pressure, masking autistic traits, untreated ADHD, relationship stress, and physical illness can all shape when symptoms appear and how severe they become.
Practical rule: Treat genetics as a vulnerability factor, not a sentence.
That's the heart of the anxiety disorder genetic question. The inherited piece is real. It just isn't the whole story.
What We Know from Anxiety Disorder Genetic Research
The biggest misconception in this area is the idea of a single “anxiety gene”. That isn't how anxiety works.
Current research points to polygenic risk. That means many genetic variants contribute, each with a small effect. No individual variant can diagnose anxiety, explain a person's whole clinical picture, or tell you which treatment will work. What these variants do is shift vulnerability across biological systems that affect threat detection, arousal, inhibition, and emotional regulation.
What large studies have found
A 2026 genome-wide association study of 122,341 European-ancestry cases and almost 730,000 controls identified 58 independent genetic loci linked to major anxiety disorders, and it highlighted GABAergic signaling as a key biological pathway (report on the 2026 anxiety genetics study). That finding supports what clinicians already see. Anxiety doesn't come from one broken switch. It reflects many small shifts across brain systems involved in inhibition and fear regulation.
GABAergic signalling matters because GABA is central to how the brain dampens excessive activity. When this pathway appears in anxiety genetics research, it gives biological context to symptoms people describe in ordinary language. “I can't settle.” “My body stays keyed up.” “My mind doesn't stop scanning for danger.”
What works and what doesn't when interpreting this research
The useful interpretation is measured. Genetics research helps us understand vulnerability and biology. It may eventually improve risk modelling and refine treatment development. It does not currently give individuals a stand-alone clinical answer.
What doesn't work is over-reading the science:
- It doesn't support direct-to-consumer diagnostic claims: A DNA test cannot tell you whether you have an anxiety disorder.
- It doesn't replace psychiatric formulation: Symptoms still need to be understood in context.
- It doesn't untangle overlap by itself: Genetics can't tell you whether poor concentration comes from ADHD, anxiety, autistic overload, depression, or a combination.
The science is strongest when it explains why anxiety is complex. It becomes weak when people use it to promise simple answers.
For patients, that's often disappointing at first. Then it becomes reassuring. If there isn't one anxiety gene, there also isn't one fixed genetic destiny.
The Genetic Overlap of Anxiety ADHD and Autism
Many adults finally recognise themselves. They've spent years trying to decide whether their difficulty is “really” anxiety or “really” ADHD or “really” autism, when the more accurate answer may be that these conditions overlap biologically and clinically.
A major genetic study involving more than 1 million participants found significant genetic overlap between anxiety and other psychiatric conditions including depression, schizophrenia, bipolar disorder, PTSD, and suicide-related traits (Yale summary of the anxiety genetics findings). That doesn't give us a simple one-to-one map for ADHD and autism, but it does support the broader clinical reality that psychiatric diagnoses don't exist in sealed compartments. Shared biology is common.
Why overlap creates diagnostic confusion
ADHD can produce chronic underperformance, forgetfulness, emotional volatility, and repeated experiences of getting things wrong. Over time, many people become anxious because life feels unpredictable and effort doesn't reliably lead to results.
Autism can bring sensory overload, social uncertainty, rigid coping routines, and exhaustion from masking. Anxiety may then build around change, social exposure, or environments that feel impossible to control.
The reverse also happens. Severe anxiety can make a person appear inattentive, avoidant, restless, or socially awkward. That's why quick self-labelling often misses the mark.
| Symptom/Trait | Anxiety Disorder Manifestation | ADHD Manifestation | ASD Manifestation |
|---|---|---|---|
| Attention problems | Worry pulls focus away from tasks | Distractibility and difficulty sustaining attention | Focus may narrow or shift under overload |
| Restlessness | Physical tension, panic, inability to relax | Hyperactivity or internal mental restlessness | Agitation may appear during sensory or social strain |
| Social difficulty | Fear of judgement, avoidance, anticipatory worry | Interrupting, missing cues, impulsive speaking | Difficulty reading social rules, reciprocity, or subtext |
| Emotional overwhelm | Catastrophic thinking, persistent apprehension | Rapid frustration, poor regulation, rejection sensitivity | Shutdown, distress with change, overload responses |
| Avoidance | Staying away from feared situations | Avoiding tasks that require sustained effort | Avoiding unpredictable, sensory-heavy, or socially complex settings |
What specialist assessment tries to separate
The core question isn't whether symptoms look similar. They often do. The key question is what drives them.
A clinician will usually look at:
- Timing: Did these traits exist from early life, or did they emerge after anxiety became severe?
- Context: Are difficulties present across settings, or mostly in feared situations?
- Function: Is the person avoiding because they're overwhelmed, because they're distracted, because they fear judgement, or because all three happen together?
If you're trying to make sense of that overlap, good guidance on neurodiversity and mental health support can be a helpful companion to formal assessment.
For a more direct look at how conditions commonly cluster in practice, this overview of comorbidities with ADHD reflects the sort of complexity that specialist services assess routinely.
How Genetics Inform a Clinical Assessment
Family history is useful in clinic, but not in the way people often fear. It isn't there so a psychiatrist can “predict your future” or reduce you to your relatives. It's there because patterns across generations can clarify what kind of vulnerability may be present.
If someone presents with chronic anxiety, concentration problems, shutdown under pressure, and social difficulty, I want to know whether similar themes have appeared in parents, siblings, or children. Not because family history decides the diagnosis, but because it helps me weigh competing explanations.
What a psychiatrist actually does with family history
A proper psychiatric assessment uses family history alongside developmental history, current symptoms, educational or occupational functioning, physical health, and life events. The process is cumulative. One detail rarely settles the matter. The pattern does.
For example, if anxiety appears alongside longstanding sensory sensitivity, rigid routines, social confusion from childhood, and relatives with similar traits, autism may need careful consideration. If the story is one of lifelong disorganisation, inconsistent attention, emotional impulsivity, and repeated stress from missed demands, ADHD may be part of the picture. If symptoms began after a specific period of panic, trauma, or prolonged stress, anxiety itself may be the main driver.
A structured psychiatric assessment is designed to distinguish those possibilities rather than collapsing them into a single label too quickly.
What helps assessment and what muddies it
The most useful preparation is practical, not dramatic:
- Bring a simple family map: Note relatives with diagnosed conditions, marked anxiety, chronic avoidance, probable ADHD traits, autistic traits, addiction, or major mood problems.
- Track developmental clues: School reports, old comments about distractibility, shyness, rigidity, behaviour, or social communication can be surprisingly informative.
- Describe your worst periods clearly: What triggered them, how long they lasted, and what changed functionally.
What tends to muddy the picture is retrospective over-interpretation. Once people start reading online, every trait can begin to look diagnostic. That's understandable, but it can flatten the differences between anxiety-based avoidance, ADHD-related inconsistency, and autistic overload.
A good assessment doesn't ask, “Which label do you prefer?” It asks, “Which explanation best fits your developmental history and current presentation?”
Genetics informs that work. It adds context. It doesn't overrule clinical judgement.
The Future of Genetic Testing and Polygenic Risk Scores
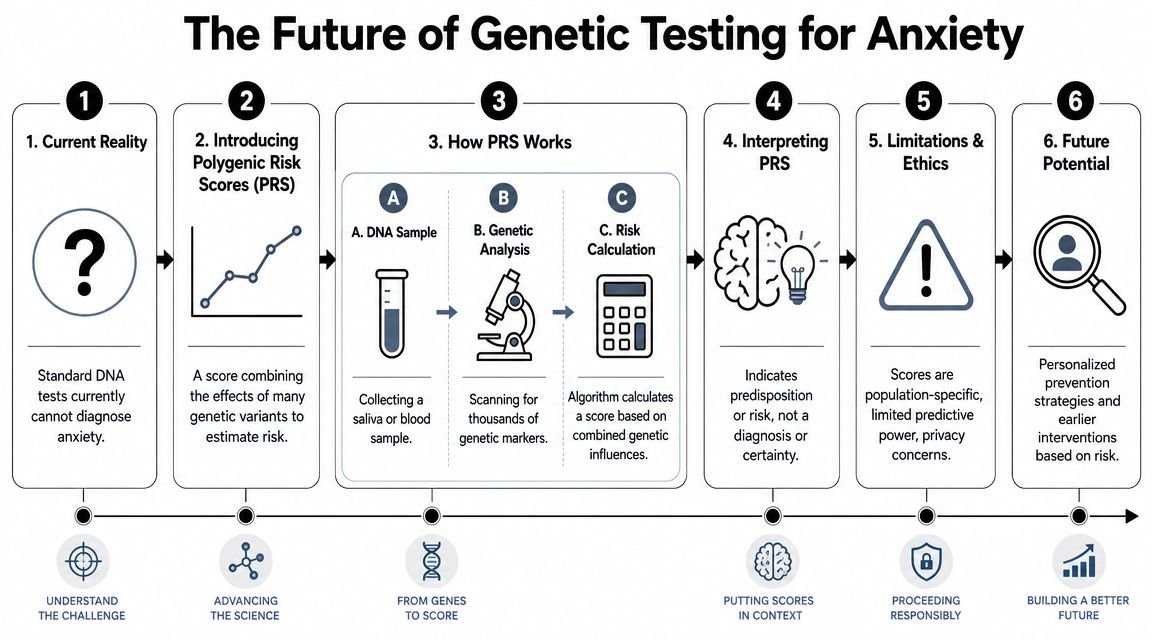
Many people now ask whether a DNA test can confirm anxiety. At present, the answer is no.
What researchers are developing instead are polygenic risk scores, often shortened to PRS. These scores combine the small effects of many genetic variants into an overall estimate of risk. That sounds impressive, and scientifically it is. Clinically, though, it's still limited.
What PRS can and can't do
A recent cross-ancestry analysis of over 1.2 million participants found that polygenic risk scores built in European ancestry samples were still associated with anxiety in African, Admixed-American and East Asian groups, but the research base remains heavily shaped by European datasets, raising concerns about accuracy and fairness (cross-ancestry anxiety genetics analysis).
That finding is important for UK patients because clinical services increasingly work with multi-ethnic populations. A risk tool developed mainly from European datasets may have uneven performance across ancestry groups. So even when a score shows some transferability, interpretation remains cautious.
Here's the practical position:
- PRS may indicate statistical predisposition: They do not diagnose an anxiety disorder.
- They don't replace interview-based assessment: They can't tell you why symptoms developed, what they mean, or what support you need now.
- They raise ethical questions: Privacy, interpretation, and fairness all matter, especially if people start treating risk scores as certainty.
Where the hype gets ahead of the evidence
The public conversation often jumps from “researchers found genetic markers” to “personalised mental health DNA tests are here”. That leap is premature.
What may become useful in future is layered medicine. Genetics might eventually sit alongside symptom history, developmental assessment, medication response, and psychological formulation. Even then, it's unlikely to replace clinical judgement. It will probably add another strand of evidence.
Some readers exploring the genetics side of treatment decisions may also find this discussion of optimizing mental health medications useful, particularly as a contrast between pharmacogenomic testing and the very different question of diagnosing anxiety through genetics.
Research tools can be powerful without being ready for routine diagnosis. That's where anxiety genetics stands right now.
The anxiety disorder genetic field is moving fast, but a careful adult should be wary of any service promising certainty from a saliva sample.
Your Next Steps for Understanding Family Mental Health
If this article has clarified anything, it should be this. Genetics can shape vulnerability to anxiety, but they don't provide a stand-alone explanation for why you feel the way you do. Anxiety, ADHD, and autism can overlap in ways that are hard to separate without specialist assessment. Family patterns are informative, not definitive.
A practical way to move forward
Start by writing down what you know, not what you suspect. Keep it simple.
- Note family patterns: Anxiety, panic, chronic avoidance, attentional problems, autistic traits, mood instability, or longstanding social difficulty.
- Record your own timeline: Childhood traits, school difficulties, sensory issues, concentration problems, social patterns, and when anxiety became impairing.
- Focus on function: Where are things breaking down now. Work, relationships, sleep, routines, confidence, or daily tasks.
If questions persist, seek a thorough adult assessment from a clinician who understands both mental health and neurodevelopmental presentations. That matters because treatment depends on formulation. Anxiety driven by panic, anxiety driven by autistic overload, and anxiety that develops secondary to untreated ADHD may look similar from the outside, but they often need different support.
You don't need to solve the whole family puzzle before asking for help. You only need enough information to begin the conversation well.
If you want a structured, consultant-led evaluation, Insight Diagnostics Global provides thorough adult assessments for ADHD, autism, anxiety, and related mental health concerns. Their service is CQC regulated, led by psychiatrists on the GMC Specialist Register, and offers clear triage, detailed reports, personalised recommendations, and optional follow-up support for adults seeking diagnostic clarity.