

You may be at one of two points.
You're either already practising and trying to decide whether your next move should be an NHS consultant post, a hybrid portfolio, or a specialist neurodevelopmental role. Or you're looking at the UK from abroad, seeing genuine opportunity, but also a maze of registration rules, training language, service models, and unfamiliar hiring processes.
Both reactions are sensible. The UK offers real scope for psychiatrists, especially those with credible experience in Autism, ADHD, complex assessment, and the overlap between neurodevelopmental presentations and wider mental health needs. But psychiatrist jobs in the UK aren't won by broad enthusiasm alone. They're won by understanding where the pressure points are, what services need, and how to present your experience in the terms the system recognises.
In practice, the strongest candidates don't just ask, “Are there jobs?” They ask better questions. Which services are short of consultant-level decision-makers? Which roles involve straightforward follow-up work, and which require high-quality diagnostic formulation? Which employers support careful assessment, and which are trying to process demand faster?
If you're weighing those questions now, a practical overview of what working as a psychiatrist can look like in a specialist setting is this guide to a job as a psychiatrist. It helps frame the move not as a generic job search, but as a deliberate career choice.
Setting the Stage for Your UK Psychiatry Career
A common pattern I see is this. A good psychiatrist starts searching for roles and quickly finds plenty of adverts, yet still feels unclear. The titles sound familiar, but the actual work varies sharply. One “consultant psychiatrist” post may be heavily rota-driven and service-pressured. Another may be centred on structured assessment, formulation, and senior clinical judgement.
That difference matters most in neurodevelopmental work.
Autism and ADHD services aren't just “general psychiatry with a different label”. The best roles demand accuracy with developmental history, confidence with diagnostic uncertainty, awareness of differential diagnoses, and the ability to separate trauma, personality structure, mood instability, anxiety, substance use, and executive dysfunction from core neurodevelopmental traits. If you miss that nuance, you won't enjoy the work, and the service won't get what it needs.
What talented psychiatrists often get wrong early
Many applicants focus too much on the employer brand and too little on job design. They ask whether the role is NHS or private, full-time or part-time, remote or face to face. Those questions matter, but they're secondary.
Start here instead:
- Clinical depth: Will you be expected to make independent diagnostic decisions in Autism and ADHD, or mostly implement pathways designed by others?
- Assessment model: Does the service use proper multidisciplinary input, psychological assessment where indicated, and clear report standards?
- Complexity tolerance: Will the team support mixed presentations involving personality difficulty, affective symptoms, trauma history, or diagnostic ambiguity?
- Governance: Is there a serious approach to documentation, consent, prescribing boundaries, and safeguarding?
The best post on paper can still be the wrong post for you if the clinical model is thin.
Why neurodevelopmental psychiatry is different
In generic job searches, Autism and ADHD work is often treated as a narrow niche. It isn't. It sits at the intersection of adult mental health, developmental psychiatry, psychological assessment, risk evaluation, and long-term functional planning.
That's why experienced psychiatrists often find this area professionally satisfying. Done well, the work is careful and intellectually honest. You're not only assigning diagnoses. You're deciding what the diagnosis explains, what it doesn't explain, and what support or treatment should follow.
Understanding the UK Psychiatry Job Market
A psychiatrist reviews two consultant posts in the same week. Both mention ADHD and autism. One is a high-volume diagnostic line with little time for formulation, limited supervision, and unclear prescribing rules. The other has slower throughput, stronger MDT input, clear report standards, and consultant control over complex decisions. On paper, both sit in the same market. In practice, they are very different jobs.
That distinction matters because the UK market remains under pressure. The Royal College of Psychiatrists reported in its 2023 workforce census that consultant vacancies and locum dependence remain high, with a true vacancy rate of 28.6% once vacant and locum-covered posts are counted together, according to the Royal College of Psychiatrists workforce census 2023.
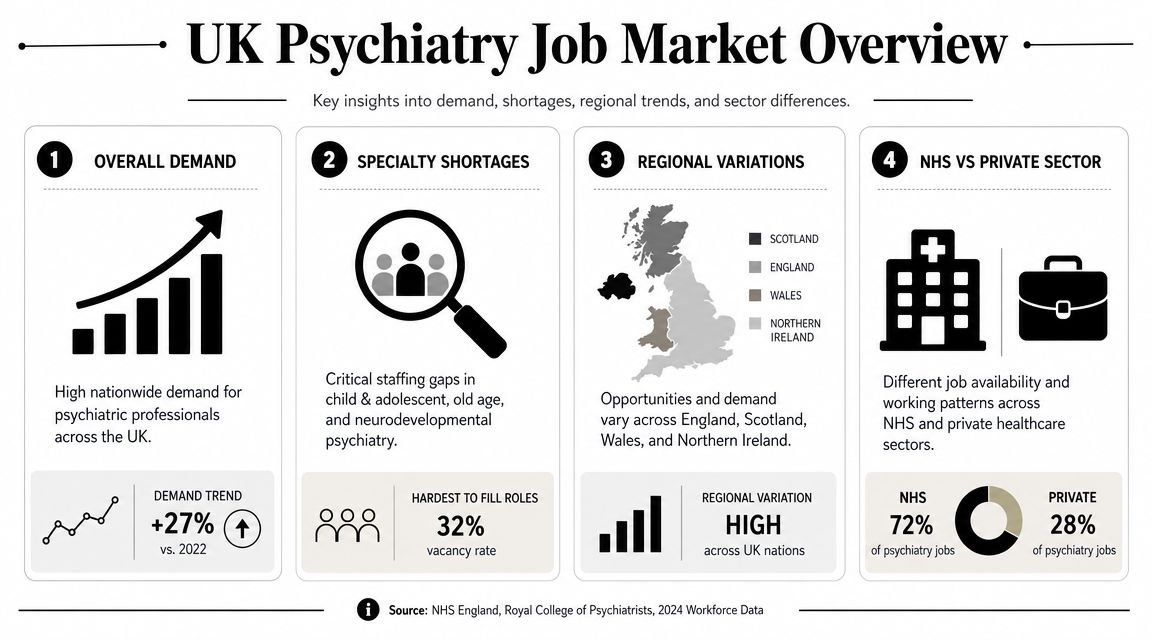
High vacancy rates do not mean every post is attractive. They mean services are competing for psychiatrists while trying to manage waiting lists, governance demands, and increasing case complexity. In neurodevelopmental work, that pressure often shows up in job design before it appears in the advert. The key question is not only whether a service needs you. It is whether the service will let you practise properly.
That is why the strongest opportunities often sit in expert-led autism and ADHD services rather than in generic vacancies alone. Good neurodevelopmental roles ask for consultant judgement in differential diagnosis, comorbidity, risk, functional impact, and treatment planning. We see this clearly in services such as Insight Diagnostics, where the work depends on careful assessment rather than simple pathway processing. If you want long-term satisfaction in this field, look closely at whether the post gives you real authority over diagnosis, report quality, prescribing decisions, and clinical boundaries.
A practical reading of the market looks like this:
| Area | What it usually means for applicants |
|---|---|
| General NHS consultant roles | Wider availability, but often higher service pressure, heavier on-call commitments, and less control over clinic structure |
| Hard-to-fill sub-specialties | Better prospects for doctors with a clear niche and evidence of independent senior practice |
| Neurodevelopmental services | Rising demand for psychiatrists who can assess ADHD, autism, overlap with trauma or mood disorder, and diagnostic uncertainty |
| Hybrid and digital services | Greater flexibility, but only attractive if governance, consent, documentation, and prescribing arrangements are clearly defined |
Regional variation still matters, but specialty fit matters more. A well-built neurodevelopmental post in a less fashionable location can be better for your development than a brand-name role with weak supervision and blunt throughput targets.
NHS and private work also overlap more than many applicants expect. Some NHS posts offer excellent multidisciplinary assessment and serious consultant leadership. Some private and independent services offer better pacing, cleaner governance, and more time to write reports that stand up to scrutiny. Others are commercially busy and clinically thin. The label does not answer the question. The operating model does.
That is one reason experienced psychiatrists often move toward specialist autism and ADHD services after years in broader adult work. The work is demanding in a different way. You need to tolerate ambiguity, hold competing explanations in mind, and avoid over-claiming what a diagnosis can explain. In my view, that is where good neurodevelopmental psychiatry remains professionally rewarding.
For a grounded comparison of substantive, locum, and specialist earnings, this guide to how much psychiatrists make in the UK across different settings is useful. For the longer-term employment picture, Stewart Accounting's view on AI in healthcare makes a fair point. Senior psychiatric judgement, especially in formulation-heavy neurodevelopmental assessment, is difficult to automate.
Your Credentialing Pathway to the GMC Specialist Register
A common scenario looks like this. An experienced psychiatrist arrives with years of solid clinical work, good references, and real confidence in adult ADHD or autism assessment, then gets stalled by paperwork because the evidence is not mapped to UK training standards. In psychiatry recruitment, especially at consultant level, the file has to read as clearly as the clinician thinks.
The GMC Specialist Register matters because it is the point at which your experience becomes formally usable for substantive consultant work. Services may value specialist expertise, but appointing panels still look for approved training, equivalent evidence, and a clean account of how competence was gained and supervised. That is true in general adult psychiatry and it is just as true in neurodevelopmental services.
CCT and the practical meaning of the standard route
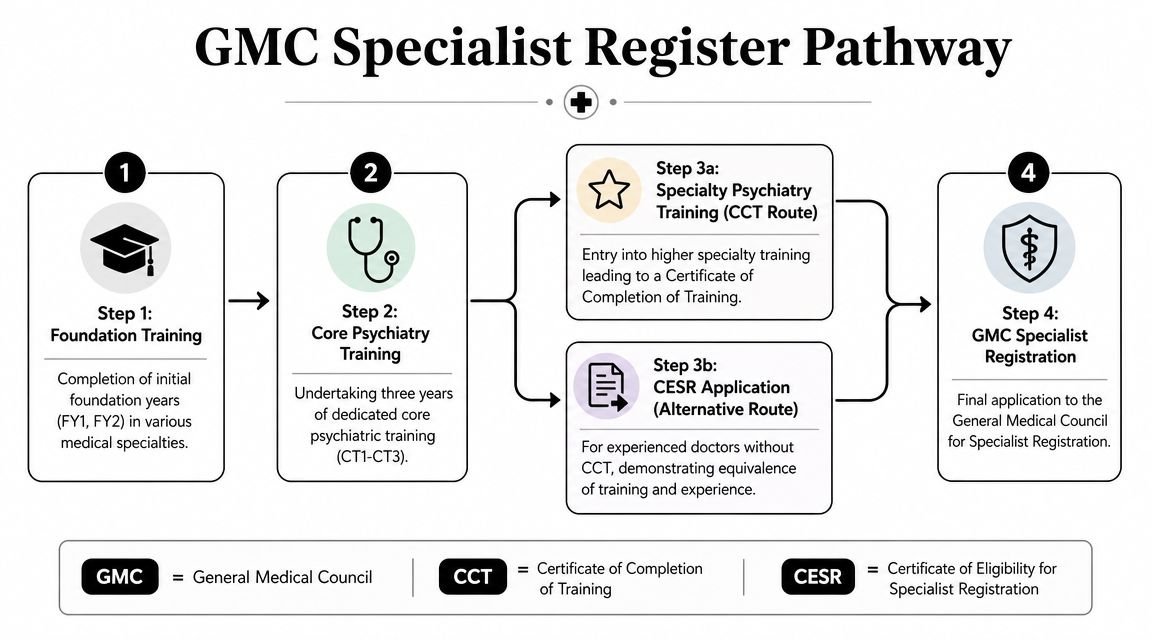
For doctors coming through UK training, the standard route is Certificate of Completion of Training, followed by entry onto the Specialist Register. On paper, the sequence is simple. In practice, each stage depends on signed evidence, workplace assessments, progression records, and supervision that matches the curriculum.
The broad pathway is familiar:
- Medical degree and foundation training
- Core psychiatry training
- Higher specialty training
- Entry to specialist registration
The pressure point is not understanding the sequence. It is producing evidence in the format UK employers, training bodies, and the GMC expect.
Here's the process in visual form:
Why international applicants often stumble
For higher training at ST4, NHS England sets out a clear process through Oriel, a standard interview, and documentary proof of core psychiatry competences, as explained in its guidance on applying for higher psychiatry training. The principle matters beyond training applications. Panels want to see that your previous work maps directly onto the UK curriculum, not that it merely sounds senior.
This catches out a lot of good doctors.
International medical graduates often focus first on GMC registration and visa status. Those matter, but they are only part of the job. The harder task is showing where you met UK standards in assessment, diagnosis, risk management, MDT working, legal awareness, communication, supervision, and clinical leadership. If that mapping is weak, your application becomes difficult to shortlist, however good your day-to-day practice has been.
A useful rule is simple. Submit mapped evidence, not a long description of experience.
What stronger evidence looks like in neurodevelopmental psychiatry
For applications, specialist applicants can either stand out or undersell themselves. Adult autism and ADHD work generates exactly the kind of evidence panels want, but only if you present it properly.
For example, if you have worked in a service such as Insight Diagnostics, or in a similar expert-led model, do not stop at saying you assessed ADHD and autism. Show the components of consultant-level practice. Describe how you took and weighed developmental history. Show how you handled competing explanations such as trauma, anxiety, mood disorder, sleep problems, substance use, or personality factors. State where you made the final diagnostic call, where you advised against diagnosis, and how your reasoning was documented and supervised.
That level of detail matters because neurodevelopmental psychiatry is formulation-heavy. A fast service can still be clinically thin. A slower service with good governance, careful collateral history, and multidisciplinary review often gives you better evidence for CESR or consultant applications than a high-volume post with little scrutiny. I have seen experienced clinicians underestimate this. Panels usually do not.
It also helps to explain your role clearly in mixed teams. If you are applying into an autism or ADHD service that uses psychologists, nurses, speech and language therapists, or occupational therapists, be precise about what the psychiatrist contributes that other disciplines do not. This summary of the difference between psychologist and psychiatrist in the UK is a useful reference point for framing that distinction.
Another practical point is service model awareness. If you have worked with NHS referral pathways, commissioned assessment contracts, or Right to Choose patients, say so. Employers in this area want clinicians who understand access routes as well as diagnosis. The Right to Choose ADHD guide gives a good overview of one pathway that increasingly shapes demand in specialist services.
For doctors outside the standard CCT route, this is usually the difference between a vague specialist profile and a credible one. Clear evidence, tied to curriculum standards and grounded in real neurodevelopmental work, is what gets you taken seriously.
Targeting Roles in ADHD and Autism Services
This is one of the most interesting parts of the current market. Neurodevelopmental psychiatry has moved from a peripheral interest to a central area of service demand. But not every role advertised under Autism or ADHD is built well.
Some posts are triage-heavy throughput roles. Others involve proper consultant work: reviewing complex histories, clarifying differential diagnoses, deciding when a diagnosis is justified, contributing to integrated reports, and managing medication or follow-up where appropriate.

What good neurodevelopmental work looks like
In a serious service, adult Autism and ADHD assessment isn't a single interview followed by a rapid conclusion. It involves triangulation.
That usually includes:
- Developmental history: Not as a formality, but as the backbone of the formulation.
- Current functioning: Work, study, relationships, sensory profile, organisation, burnout patterns, and adaptive strategies.
- Differential diagnosis: Mood disorder, anxiety disorder, trauma-related presentations, personality difficulty, sleep disorder, substance use, and cognitive issues.
- Psychological assessment input: Often decisive when presentations are subtle, compensated, or clinically tangled.
- Clear report writing: Diagnostic reasoning must be explicit, not implied.
This is why some psychiatrists thrive in these settings and others don't. You need patience with ambiguity. You need to be comfortable saying, “This may be ADHD, but I need more evidence,” or “There are autistic traits here, but they don't yet justify a full diagnostic conclusion.”
The role of consultant-led services
A growing part of the market sits in consultant-led, CQC-regulated services that combine psychiatric review with structured psychological assessment. That model suits clinicians who prefer depth over volume.
In those settings, psychiatrists often work alongside psychologists and wider clinical teams rather than acting as isolated diagnostic gatekeepers. For candidates with interests in personality structure, trauma, emotional dysregulation, and neurodevelopmental overlap, that can be a strong fit. It's also why experienced neurodevelopmental and personality disorder clinicians, including senior consultants such as Dr Sai Achuthan, are well placed in this field. The work rewards nuanced formulation rather than narrow checklist practice.
In adult ADHD and Autism work, the difficult cases are usually the ones with several partially true explanations competing at once.
Remote and hybrid roles need closer scrutiny
The UK job market is also being reshaped by digital delivery. Many psychiatrist postings now include remote or hybrid work, but those adverts often skip the most important questions: workload design, safeguarding arrangements, prescribing boundaries, supervision, and medico-legal risk, as reflected in the service model discussion at Psychiatry UK careers.
A remote role can be excellent. It can also be a poor fit if the service expects consultant-level responsibility without enough administrative support, governance structure, or protected time for documentation.
When reviewing these posts, ask:
- Who owns the pathway? Are you shaping assessment decisions or just signing off them?
- How is safeguarding handled? Especially when risk emerges during a virtual assessment.
- What happens after diagnosis? Is there follow-up, titration, signposting, or discharge?
- How are reports quality-assured? This tells you a lot about the seriousness of the service.
Patients often approach these pathways through alternative access routes, so it helps to understand the policy context. This Right to Choose ADHD guide offers a clear patient-facing explanation of one such route, and this summary of NHS Right to Choose ADHD pathways is useful if you want to understand how referral demand reaches specialist services.
Mastering the Application and Interview Process
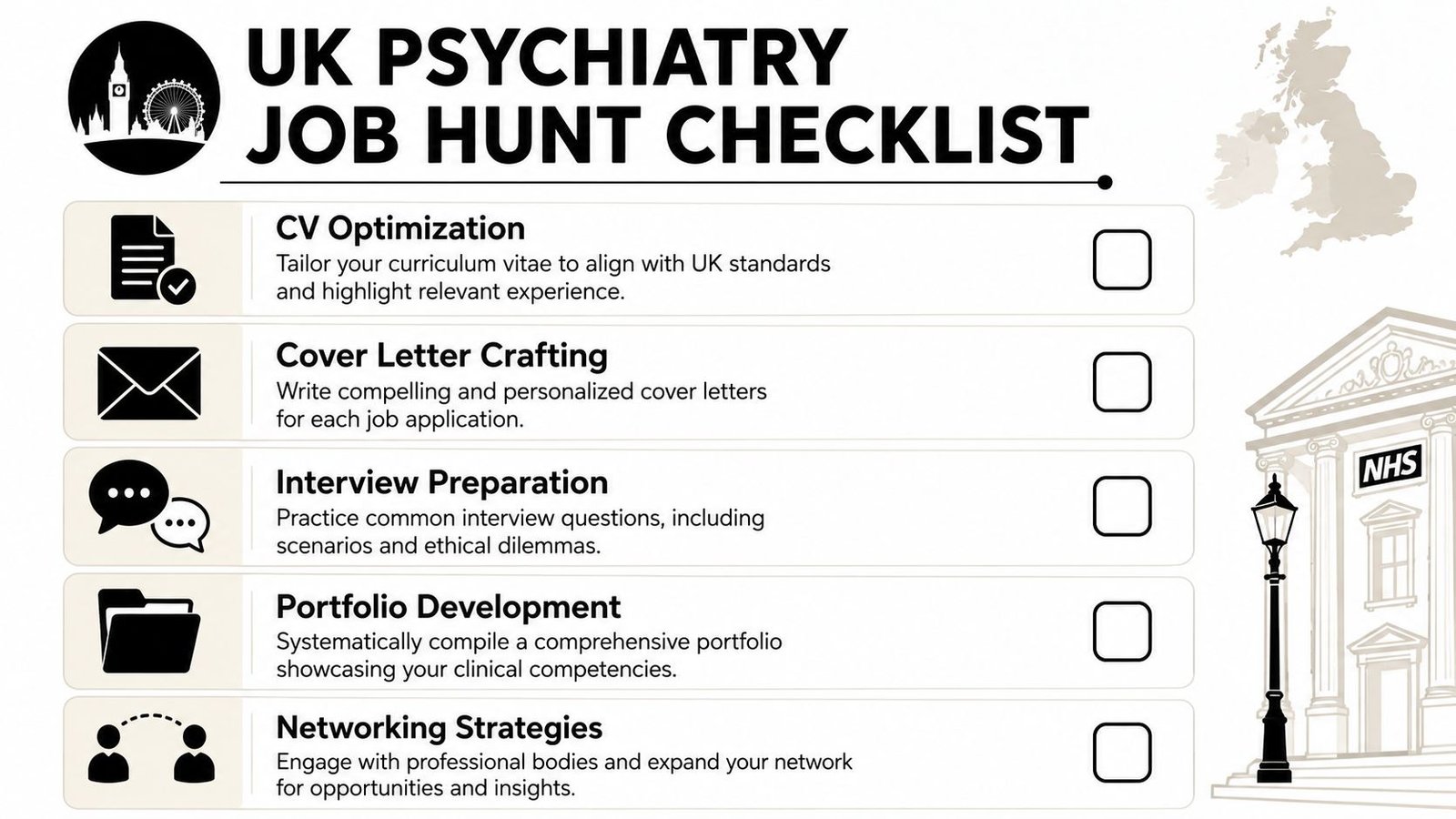
A strong psychiatrist CV in the UK doesn't read like an autobiography. It reads like evidence. Employers want to know what you can safely and independently do, in what setting, with what level of complexity, and with what governance awareness.
That's particularly true if you're applying across sectors or translating overseas experience into UK terms.
Build a UK-ready CV
The mistake I see most often is overloading the document with roles and under-explaining competence.
A better approach is to organise around clinically relevant proof:
- Scope of practice: State your sub-specialty exposure clearly. Adult, CAMHS, liaison, neurodevelopmental, rehabilitation, old age, or mixed.
- Decision-making level: Specify whether you assessed independently, supervised juniors, led MDT discussions, or contributed to service development.
- Assessment and treatment detail: Mention Autism and ADHD assessment, medication management, risk assessment, tribunal work, Mental Health Act experience, or report writing where applicable.
- Governance evidence: Audit, teaching, supervision, complaint handling, quality improvement, and documentation standards all count.
If you want a non-medical but useful reminder of how sharply written CVs differ from weak ones, this guide on how to create a job-winning resume is worth reading for structure and clarity alone.
Search like a strategist
The UK market has a geographic and specialty mismatch between where psychiatrists are available and where vacancies are highest. Smart applicants look beyond headline numbers and identify the regions and sub-specialties with persistent gaps, particularly in areas such as child, adolescent, and liaison psychiatry, as discussed in the earlier linked workforce overview of regional and specialty pressures.
That should change how you search.
Use three lenses:
| Search lens | What to ask |
|---|---|
| Region | Is this an area where recruitment is difficult, which may improve leverage and progression? |
| Sub-specialty | Does the service need your exact experience, or just any consultant? |
| Job design | Is the role sustainable, or is it compensating for chronic under-structure? |
Interview for the service, not the title
A UK psychiatry interview usually tests whether you can function safely inside a real service. Clinical knowledge matters, but practical judgement matters more.
Expect questions around:
- Complex clinical formulation
- Risk and safeguarding
- Team conflict or disagreement
- Clinical governance
- Why this service, not just this specialty
Prepare examples that show your thinking process. In neurodevelopmental roles, be ready to discuss diagnostic overlap, contested diagnoses, patient expectations, and situations where a careful non-diagnosis was the right outcome.
If your answer only shows knowledge, you sound junior. If it shows judgement, boundaries, and service awareness, you sound appointable.
Private-sector interviews often add questions about pace, report turnaround, patient communication, and remote assessment standards. NHS interviews may push harder on leadership, service pressure, and interface working. In both settings, clear examples beat polished abstractions every time.
Negotiating Your Contract and Finalising Your Move
A weak contract can turn a good-looking consultant post into daily frustration within three months. I see this most often in ADHD and autism services, where employers advertise for specialist judgement but build the role around volume, thin admin support, and unrealistic turnaround times.
Once the offer arrives, the key question is simple. Is this a consultant job, or a senior clinician post dressed up as one?
In neurodevelopmental psychiatry, that distinction matters. A properly designed role gives you time for triage, diagnostic formulation, collateral review, report writing, risk work, and difficult conversations when the right outcome is no diagnosis or a more cautious differential. A poorly designed role assumes assessment slots alone are the job. That usually means pressure on quality, higher complaint risk, and consultant time being spent firefighting process failures.
Salary still matters, but experienced psychiatrists rarely regret negotiating for structure. They do regret accepting vague promises.
Focus on the parts of the contract that determine whether the work is clinically defensible:
- Session design: How many direct assessments, report sessions, MDT meetings, and admin sessions are built into the job plan?
- Report expectations: Who sets turnaround times, what length and standard are expected, and is there protected time to produce work you are willing to sign?
- Clinical support: Is there skilled case coordination, secretarial input, and a pathway for gathering school, family, or collateral information?
- Decision-making authority: Can you shape diagnostic thresholds, follow-up recommendations, and prescribing boundaries, or are these effectively fixed by management?
- Remote practice arrangements: Are platforms, indemnity arrangements, prescribing processes, and information governance already in place?
- CPD and peer review: Is there funded study leave, appraisal support, and regular consultant-level discussion of complex autism and ADHD cases?
- Portfolio flexibility: If you want a mixed NHS and independent career, check for any contractual restrictions early.
The trade-off is straightforward. Higher sessional pay can be offset by poor infrastructure. Lower headline pay in a well-run service can produce better clinical work, fewer complaints, and a career that remains enjoyable.
This is especially true in specialist independent services. At Insight Diagnostics, for example, the attraction is not just the subject matter. It is the combination of consultant-led assessment, structured pathways, clear reporting standards, and work that respects the complexity of adult neurodevelopmental presentations. That kind of setup suits psychiatrists who care about careful diagnosis rather than throughput alone.
If you are relocating from overseas, handle the practical points at the same time as contract review. Confirm visa sponsorship, GMC status, indemnity, start date, and whether the post is conditional on references or further documentation. Ask who is responsible for each step. Services that recruit international psychiatrists regularly will answer clearly and in writing.
Then do one final sense-check. If the role expects independent diagnosis, complex formulation, medication decisions, safeguarding judgement, and polished documentation, the contract should show where the time and support for that work sit.
If it does not, keep asking questions before you sign.
If you're looking for a consultant-led setting in adult Autism, ADHD, and broader mental health assessment, Insight Diagnostics Global is worth exploring. The service offers online and face-to-face assessments for adults, with GMC Specialist Register psychiatrists, structured diagnostic pathways, clear reporting, ADHD titration and follow-up, and a model that values careful triage and clinical rigour. For psychiatrists who want work that combines neurodevelopmental expertise with high-quality assessment practice, it's the kind of service model that deserves a close look.