

Considering a mental health assessment can feel daunting. You might be wondering what you'll be asked, whether you'll say the “right” thing, or what happens if your answers point to ADHD, autism, anxiety, depression, or more than one difficulty at once. That uncertainty is common, especially if you've spent a long time masking, second-guessing yourself, or being told your struggles are “just stress”.
A good assessment isn't an exam. It's a structured, collaborative clinical conversation that helps a specialist understand your experience in context. In England, the scale of need is high. The Adult Psychiatric Morbidity Survey reported that 1 in 6 adults had a common mental disorder in 2014, which is one reason careful early questioning matters so much in real services.
For adults seeking clarity around ADHD, autism, and mental health together, the questions matter because the overlap matters. Poor concentration can reflect ADHD, anxiety, burnout, depression, trauma, sleep problems, or several of these at once. Social exhaustion can point towards autism, but it can also arise from chronic anxiety or low mood. Consultant-led services such as Insight Diagnostics Global, including specialists with neurodevelopmental expertise such as Dr Sai Achuthan, use assessment questions to sort through that complexity with care. The aim is clarity, not labels for their own sake.
1. General & Background Questions. Setting the Scene
The opening part of an assessment often feels broad. That's deliberate. A clinician usually starts with your current concerns, your living situation, work or study, relationships, physical health, medication, and any previous support you've had. These questions create the frame for everything that follows.
A short symptom checklist on its own can miss too much. If someone says they're exhausted, losing focus, and feeling overwhelmed, the meaning changes depending on whether they're a university student under pressure, a parent barely sleeping, an adult with long-standing ADHD traits, or someone whose mood has shifted after a major life event.
Why clinicians start wide
General questions help identify patterns, timing, and context. They also help a psychiatrist decide whether a difficulty looks longstanding, recent, situational, or part of a broader condition. That matters in neurodevelopmental work, because ADHD and autism aren't judged only by what's happening this month. The developmental story matters.
A clear explanation of the process can make this stage much easier, and Insight Diagnostics Global's guide to what a mental health assessment involves is useful if you want to see how a structured UK pathway is usually described before booking.
Practical rule: Don't try to sound “serious enough” or “not too serious”. The most helpful answers are plain, concrete ones.
You don't need polished language. “I'm late for everything, my inbox is chaos, and I avoid calls because I dread them” is often more useful than a vague “I'm struggling”.
For some adults, memory or cognitive concerns also sit in the background of an assessment, especially when stress, ageing, sleep disruption, and mood overlap. In those cases, broader context is important too, including the kind of practical family observations discussed in Family Caregiving Kit's memory care advice.
2. Mood & Anxiety Questions. Gauging Your Emotional Climate
A common assessment moment goes like this. Someone books expecting to talk about focus or burnout, then realises half the early questions are about worry, sleep, irritability, panic, loss of interest, or feeling flat. That can feel off target. Clinically, it is not.
Mood and anxiety questions help clarify what is driving the difficulty in front of you. A person who cannot concentrate may have ADHD. They may also be stuck in a cycle of hypervigilance, poor sleep, low mood, or panic. In practice, these patterns often overlap, which is why consultant-led services do not rely on one headline symptom.
You may be asked whether you have been feeling low, tense, hopeless, restless, tearful, numb, detached, or unable to enjoy things you usually value. The follow-up questions matter just as much. How often does it happen? When did it start? Is there a trigger? What changes on better days? Dr Sai Achuthan and other experienced psychiatrists use this level of detail to separate a short-term stress response from a depressive or anxiety disorder, and to see whether ADHD or autistic burnout may also be part of the picture.
The clinician is listening for pattern, not performance.
That includes severity, duration, physical symptoms, and effect on day-to-day life. For anxiety, I would usually want concrete examples. Do you avoid calls, leave messages unread, wake with dread, replay conversations for hours, or need a long recovery period after routine appointments? If someone says, “I'm anxious all the time,” the next step is to make that clinically usable.
You can see how this is explained in a UK setting in Insight Diagnostics Global's guide to anxiety diagnosis in the UK.
These questions also help with differential diagnosis. Anxiety can look like inattention because the mind is preoccupied. Depression can slow thinking, reduce motivation, and flatten memory. Longstanding neurodevelopmental conditions can then sit underneath both. Good assessment work keeps all three possibilities in view instead of rushing to a single label.
“I worry a lot” is a starting point. “I check emails repeatedly, sleep badly before meetings, cancel social plans, and feel sick on the way to work” gives the clinician something they can assess properly.
This is one reason high-quality services categorise questions carefully rather than running through a generic checklist. For patients exploring ADHD in particular, broader support sometimes comes up alongside formal diagnosis, including lifestyle discussions such as personalized supplement recommendations for ADHD. That does not replace psychiatric assessment, but it reflects a real clinical trade-off. Symptoms can have more than one contributing factor, and management often works best when the full picture is understood.
If you are unsure how to answer, be specific and plain. “I cry in the car before work twice a week” is more useful than “work stresses me out.” “I feel flat even when good things happen” is more useful than “I'm a bit down.” Clear examples reduce guesswork and help the assessment stay accurate, fair, and focused on what is affecting your life.
3. ADHD-Specific Questions. Understanding Focus & Impulsivity
Adult ADHD assessments focus on patterns, not isolated traits. Almost everyone loses focus sometimes. ADHD questions are designed to find out whether difficulties with attention, organisation, impulsivity, restlessness, and follow-through have been persistent across settings and present since earlier life.
That's why a consultant psychiatrist won't stop at “Do you struggle to concentrate?” They'll ask what concentration problems look like in practice. Do you start tasks and leave them unfinished? Miss deadlines despite caring? Interrupt people? Hyperfocus on one interest but fail to initiate routine admin? Need urgency to get anything done?
Why childhood history matters
ADHD is a neurodevelopmental condition, so developmental history is central. Adults are often asked about school reports, classroom behaviour, homework, forgetfulness, fidgeting, emotional impulsivity, and whether they were described as bright but inconsistent, dreamy, talkative, disorganised, or hard to manage.
The detail matters because many adults have adapted. They may use alarms, work late to compensate, rely on partners for organisation, or choose careers that mask symptoms. Specialist services therefore look beyond surface success. A person can be high-achieving and still significantly impaired.
If you want a practical preview of the kinds of traits often explored, Insight Diagnostics Global's adult ADHD symptoms checklist gives a useful starting point.
A common weakness in public-facing assessment content is that it explains symptoms but not the logic behind the questions. That gap matters. A review of mental health assessment tools found that some conditions are assessed with more attention to triggers than others, supporting the case for broader, more standardised assessment approaches that don't miss relevant features across the symptom spectrum in this review of 126 questionnaires and interviews.
Clinical reality: “I did well at school” doesn't rule out ADHD. Many adults compensated through intelligence, fear, structure, or family support. The question is how much effort that success cost, and whether the pattern was already there.
Some people also ask about lifestyle or nutritional strategies once ADHD is identified. Those discussions can be useful, but they sit after proper assessment, not instead of it. If that's relevant to you, personalised supplement recommendations for ADHD are best treated as adjunctive information rather than diagnosis.
4. ASD-Specific Questions. Exploring Social Interaction & Behaviour
Autism assessment questions often feel very personal because they touch on how you experience people, communication, routine, and sensory input. Adults may be asked about eye contact, conversational flow, literal interpretation, social fatigue, friendships, misunderstandings, intense interests, need for sameness, and sensitivity to sound, light, textures, or busy environments.
The point isn't to decide whether you seem “social enough”. It's to understand your natural style, the effort required to manage daily life, and whether masking has hidden longstanding autistic traits.
What specialists are looking for
An autism assessment in adults usually pays close attention to developmental history. Clinicians want to know what you were like as a child, not because they expect dramatic signs, but because autism is identified through enduring patterns. Some adults were quiet and withdrawn. Others were verbal and academically able but socially confused, rigid, or overwhelmed.
In consultant-led neurodevelopmental services, the strongest assessments don't treat autism in isolation from mental health. They ask whether social exhaustion is autistic burnout, whether repeated shutdowns have been misread as depression, and whether anxiety developed secondarily after years of trying to keep up.
Insight Diagnostics Global's guide to recognising autism in adults reflects many of the themes adults notice before formal assessment.
One of the most important developments in modern assessment is greater attention to context beyond symptoms alone. Screening guidance increasingly recommends asking about trauma exposure, poverty, racism, food insecurity, and cultural or language needs because those factors change risk and also change how symptoms should be interpreted in this screening guidance.
For autistic adults, that wider lens matters. Sensory overload, burnout, trauma, and social exclusion can all shape how difficulties present. A good assessment won't flatten those experiences into a generic checklist.
5. Risk & Safety Questions. Prioritising Your Wellbeing
You may be describing lifelong inattention, autistic burnout, panic, or low mood, then the clinician asks: “Have you felt life is not worth living?” For many adults, that is the moment the assessment feels most exposing.
A good clinician asks anyway, and asks clearly. Risk questions help us work out what needs attention first. They cover suicidal thoughts, self-harm, past attempts, current intent, self-neglect, substance use, aggression, exploitation, and whether you can stay safe at home. In a consultant-led service, this is not a scripted interruption. It is part of sound clinical reasoning.
The purpose is practical. If someone has intrusive thoughts with no intent, the response is different from someone with a specific plan, access to means, and little confidence they can stay safe tonight. The question may sound blunt, but the detail changes what happens next.
This matters in ADHD and autism assessments too.
Adults with ADHD may describe impulsive self-harm, risky spending, binge drinking, unsafe driving, or acting quickly when distressed. Autistic adults may describe shutdowns, burnout, self-injury linked to overwhelm, or becoming highly vulnerable when routines collapse. Those patterns can be misunderstood if nobody asks about risk directly and in context. Clinicians such as Dr Sai Achuthan often stress that the answer on its own is only part of the picture. Timing, triggers, frequency, planning, protective factors, and your current level of control all matter.
Clear answers help us judge urgency accurately
People often fear that saying too much will trigger an overreaction, or that minimising it will help them keep control. In practice, vague answers make decisions harder. Specific answers help the clinician match the response to the level of risk.
For example:
“I've had passing thoughts, but I don't want to act on them.”
“I've been scratching or hitting myself when overwhelmed, especially after sensory overload.”
“I'm drinking heavily, not eating properly, and I'm struggling to look after myself.”
“I have a plan, and I'm not sure I can keep myself safe tonight.”
Those are very different presentations. They should lead to different decisions.
In better assessments, risk is not reduced to suicide screening alone. We also look at exposure to abuse, coercive relationships, financial exploitation, medication misuse, and whether exhaustion or executive dysfunction has reached the point where basic safety is slipping. That wider lens is particularly important for neurodevelopmental assessments, where the immediate risk may come from overwhelm, impulsivity, or neglect rather than a conventional description of depression.
If you are asked a hard safety question, answer the question directly. You do not need polished language. Plain words are enough.
If you are in immediate danger, or you do not think you can stay safe, emergency help is the right next step rather than a routine assessment.
6. Functioning Questions. Measuring the Real-World Impact
Symptoms only tell part of the story. Functioning questions ask what those symptoms do to your life. Can you work consistently? Manage deadlines? Keep your home in order? Sustain relationships? Attend lectures? Reply to messages? Shop, cook, sleep, and pay bills without everything backing up?
The difference between a trait and a clinically significant problem becomes clearer. Many adults recognise themselves in ADHD or autism content online, but diagnosis depends partly on whether those patterns create meaningful impairment.
The questions get practical
Functioning questions are often the most revealing because they force specifics. A person may say they're “coping”, then describe chronic lateness, repeated job problems, abandoned courses, debt from missed admin, relationship strain, and total exhaustion after ordinary social contact. That isn't coping in any sustainable sense.
The strongest assessments also look at whether impairment is broad or narrow:
- Work and study impact: Missed deadlines, underperformance, avoidance, job changes, disciplinary issues, or needing extreme effort to keep up.
- Home impact: Clutter, forgotten tasks, disrupted routines, poor sleep hygiene, skipped meals, or difficulty managing appointments.
- Relationship impact: Misunderstandings, conflict, withdrawal, irritability, dependence on others for organisation, or burnout after social demands.
- Self-care impact: Hygiene, medication adherence, emotional regulation, and the ability to recover after stress.
The digital side of assessment also matters here. Online mental health screening platforms held 59.0% of global revenue in 2023, which helps explain why so many adults now start with web-based tools. But access alone doesn't solve everything. If a questionnaire is easy to open but disconnected from meaningful next steps, it won't tell the full functional story a clinician needs.
Good clinicians therefore use symptom questions and functioning questions together. That combination is what turns a generic checklist into an assessment.
7. How to Prepare & What to Expect with Insight Diagnostics Global
You sit down for an assessment and your mind goes blank. You know something has been hard for years, but turning that experience into clear examples on the spot is another matter. That is why preparation helps. It does not change your story. It makes it easier to tell accurately.
The most useful thing you can bring into an assessment is evidence of patterns. In adult ADHD and autism assessments especially, clinicians are listening for consistency across time, settings, and relationships. A single bad month matters less than a repeated pattern that shows up at school, at work, at home, or in close relationships. School reports, past referral letters, workplace feedback, notes from a partner, and a short symptom timeline can all help.
At Insight Diagnostics Global, the model is consultant-led and focused on adult presentations that are not always tidy or single-category. That matters in practice. Many adults seeking answers about ADHD or ASD also describe anxiety, low mood, burnout, trauma history, sleep problems, or long-standing difficulties with emotional regulation. A good assessment does not treat those as background noise. It examines whether they are separate conditions, consequences of years of strain, or part of the same clinical picture.
What tends to help before the appointment
A brief written summary is often more useful than trying to remember everything in real time. I usually advise patients to keep it short and concrete. Two pages is often plenty.
Useful prompts include:
- Why now: What changed recently. Worsening work demands, parenting pressures, repeated burnout, relationship difficulties, or a crisis in routine often explain why someone seeks assessment at this point.
- Early signs: Childhood concentration problems, sensory sensitivities, rigid routines, social confusion, daydreaming, impulsivity, or comments from teachers and family.
- Current examples: Missed deadlines, shutdown after social contact, forgotten appointments, overwhelm with admin, conflict caused by blunt communication, or difficulty switching tasks.
- Mental health overlap: Panic, insomnia, depressive episodes, trauma symptoms, obsessive thinking, or emotional dysregulation that may overlap with, mimic, or sit alongside neurodevelopmental conditions.
- Previous help: Medication, therapy, coaching, GP reviews, private screening, workplace adjustments, or NHS referrals.
Bring examples, not essays. Three clear examples of sensory overload, chronic lateness, or social misunderstanding usually give a psychiatrist more to work with than several pages of general reflection.
Patients also benefit from knowing the process in advance. A well-run service should explain who the assessor is, what documents are useful, whether questionnaires or collateral history are needed, how long the appointment lasts, and when to expect the report. That level of clarity reduces anxiety because it replaces uncertainty with a sequence people can prepare for.
What a consultant-led assessment should feel like
A strong assessment should feel methodical, not interrogative. The questions may be detailed, but there is a reason for that. If a psychiatrist asks about school reports, friendships, routines, driving, work performance, sleep, alcohol, panic, or family history, they are usually testing diagnostic alternatives as well as building evidence for one explanation.
That is particularly important for ADHD and ASD. Poor concentration can reflect ADHD, anxiety, depression, trauma, sleep deprivation, or several of these at once. Social withdrawal can point to autism, social anxiety, burnout, depression, or past bullying. The clinician's job is to sort pattern from overlap. Your job is to answer as plainly as you can, even if the answer feels messy.
For many UK adults, a private or insurance-funded route appeals because it allows these questions to be considered together rather than split across separate appointments and services. As noted earlier, pressure across mental health services has made clarity, continuity, and timely follow-up more important to patients. The benefit is not speed alone. It is having a coherent formulation from a specialist who can explain what fits, what does not, and what should happen next.
Be accurate. Be specific. If you mask heavily, say so. If you function well in one area but collapse afterwards, say that too. Experienced psychiatrists are listening for patterns, compensation strategies, and the difference between appearing fine and coping at a sustainable cost.
7-Point Mental Health Assessment Comparison
A useful assessment does more than collect symptoms. It shows which questions are quick screening tools, which need specialist interpretation, and which ones carry the most weight when ADHD, autism, anxiety, low mood, trauma, sleep problems, and day-to-day impairment overlap.
That distinction matters in practice. A consultant psychiatrist is not just asking more questions for the sake of it. They are weighing timing, developmental history, risk, masking, and functional impact to work out what fits best and what support should follow. In UK adult ADHD and ASD assessments, that clinical reasoning is often what patients find most reassuring once the process is explained clearly.
| Item | 🔄 Complexity & Resources | ⚡ Speed / Efficiency | 📊 Expected Outcomes | 💡 Ideal Use Cases | ⭐ Key Advantages |
|---|---|---|---|---|---|
| 1. General & Background Questions: Setting the Scene | Low complexity. Requires clinician time and basic history documents | Moderate. Quick to begin, with more time needed as detail builds | Contextual picture of life history and a starting point for diagnosis | Initial assessment, rapport-building, triage | High value for personalised formulation and differential clues |
| 2. Mood & Anxiety Questions: Gauging Your Emotional Climate | Low to moderate. Often uses standardised questionnaires such as PHQ-9 and GAD-7 with clinician review | High. Standard screens are quick to administer and score | Identification and severity grading of mood and anxiety disorders | Screening, monitoring treatment response, primary care referrals | Validated, repeatable screening with clear thresholds |
| 3. ADHD-Specific Questions: Understanding Focus & Impulsivity | Higher complexity. Needs developmental history, collateral reports, and specialist input | Lower. Assessments take longer because they review patterns across life stages | Evidence of lifelong inattention, impulsivity, and impairment across settings | Adult ADHD diagnostic work-up, medication consideration, occupational impact | Developmental focus helps distinguish ADHD from anxiety, burnout, sleep problems, and other causes |
| 4. ASD-Specific Questions: Exploring Social Interaction & Behaviour | High complexity. Requires specialist neurodevelopmental assessment, collateral history, and sensory profile | Lower. Detailed interviews and structured tools take time | Detailed profile of social communication, routines, sensory differences, and compensatory strategies | Suspected adult autism, personalised support planning, workplace or social adaptations | Detailed assessment of social and sensory patterns to guide specific interventions |
| 5. Risk & Safety Questions: Prioritising Your Wellbeing | Moderate. Requires a trained clinician, risk protocols, and sometimes urgent follow-up resources | High priority. Addressed promptly when concerns appear | Identification of immediate danger and a safety plan or urgent intervention where needed | Any assessment involving suicidality, self-harm, harm to others, or acute safety concerns | Supports immediate protection and clear duty-of-care action |
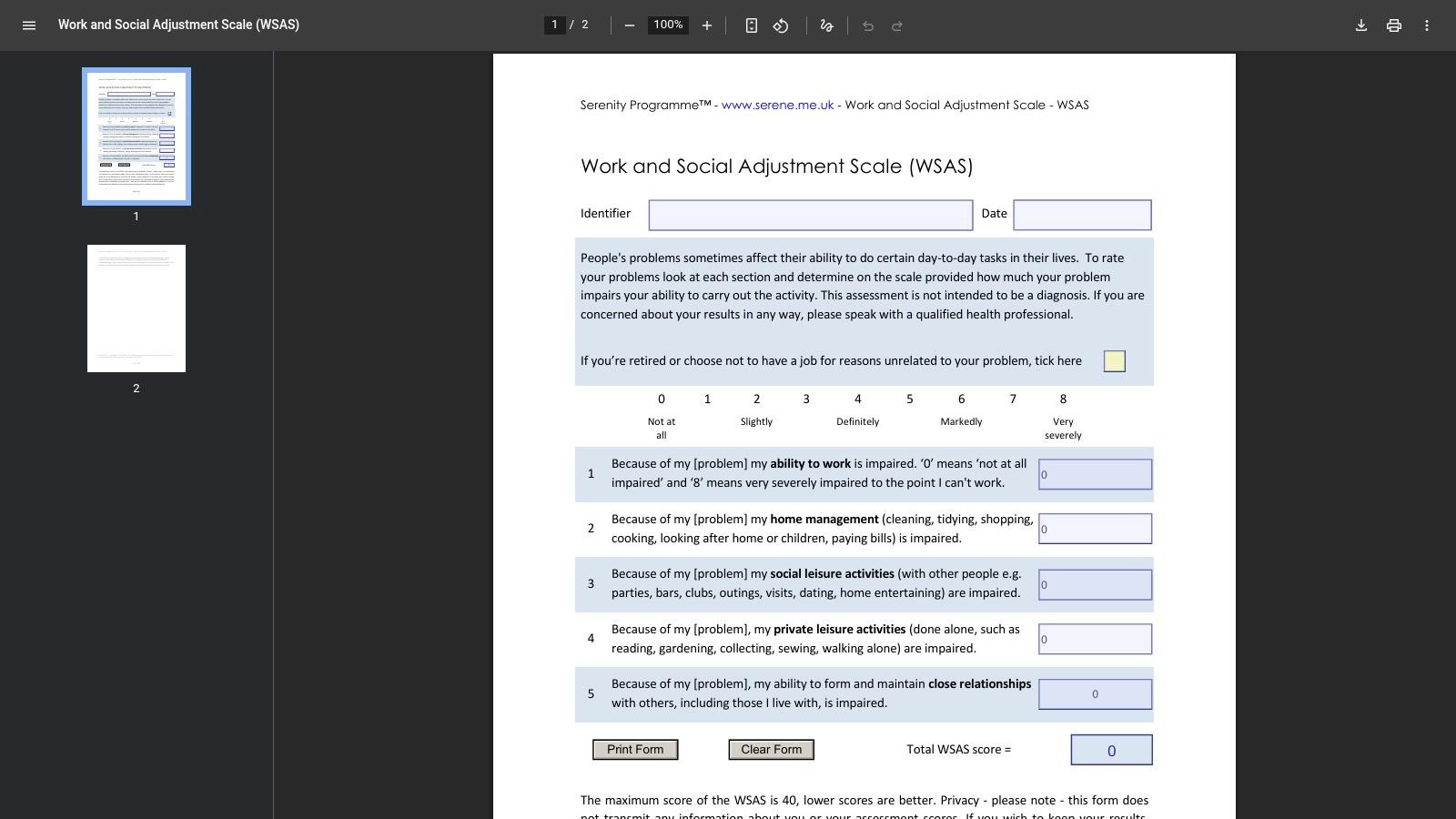
| 6. Functioning Questions: Measuring the Real-World Impact | Moderate. May include formal scales such as WSAS and practical examples from daily life | Moderate. Structured, but not usually urgent | Measurement of impairment across work, relationships, home life, and leisure. Supports treatment planning | Determining severity, benefits evidence, rehabilitation planning | Connects symptoms to day-to-day impact so priorities are practical, not abstract |
| 7. How to Prepare & What to Expect with Insight Diagnostics Global | Low to moderate. Involves patient preparation, documentation, and a consultant-led pathway | High. Streamlined triage, scheduled assessment, and prompt reporting | Clear diagnostic outcome, personalised feedback, and evidence-based recommendations | People seeking a fast, structured, consultant-led assessment pathway | Transparent process with timely, clinically useful reports |
A service such as Insight Diagnostics Global stands out when it combines speed with enough consultant time to examine overlap properly. That is particularly relevant in adult ADHD and ASD work, where surface-level answers can be misleading and where clinicians such as Dr Sai Achuthan look closely at developmental history, present-day functioning, and the cost of masking or compensating.
Your Assessment. The First Step Towards Understanding
Mental health assessment questions can feel intimidating before you hear them out loud. Once you understand the purpose behind them, they usually make much more sense. Clinicians aren't trying to catch you out. They're trying to understand how your mind works, how long the difficulties have been present, what else may be contributing, and what support is most appropriate.
That's particularly important in adult ADHD and autism work. Concentration problems aren't always ADHD. Social difficulty isn't always autism. Burnout, trauma, anxiety, depression, sleep disruption, personality factors, and chronic stress can overlap in ways that blur the picture. Good assessment questions help separate those threads instead of collapsing them into one label.
It's also worth remembering that not every question is about symptoms alone. The strongest assessments look at context, safety, developmental history, and real-world functioning. They ask what happens at work, at home, in relationships, and under stress. They ask what changed, what's always been there, and what effort it takes for you to appear as though you're coping.
For adults in the UK, that clarity matters because access pressures are real and waiting lists are long. A consultant-led service can offer something many people haven't had before, which is enough time and expertise to consider the whole picture properly. When the assessment is done well, even difficult questions can feel reassuring because they show that the clinician is being thorough, not dismissive.
If you're considering a private assessment for ADHD, autism, anxiety, depression, or overlapping mental health concerns, a CQC-regulated, consultant-led service such as Insight Diagnostics Global offers a clear and structured route forward. The value isn't just in getting an answer quickly. It's in getting an answer that reflects your actual life, your developmental history, and the complexity of your presentation.
A good assessment won't solve everything in a single conversation. What it does is give you a more accurate map. For many adults, that's the point where self-blame starts to lift, and more useful next steps become possible.
If you're ready for a clear, consultant-led assessment for ADHD, autism, or broader mental health concerns, Insight Diagnostics Global offers online and face-to-face appointments for adults, structured diagnostic pathways, detailed reports, and follow-up support from GMC Specialist Register psychiatrists.