

You may be at the stage where mental health is the part of medicine that holds your attention longest. You notice that some consultations feel rushed, that many patients don't fit neat textbook categories, and that conditions such as ADHD, autism, trauma, mood disorder, and personality difficulty often overlap in ways that need careful assessment rather than quick assumptions. If that sounds familiar, psychiatry may be the right branch of medicine for you.
A lot of students search for how to become a psychiatrist in the UK expecting a short answer. There isn't one. There is, however, a clear route, and if you understand the trade-offs early, you can move through it with much less confusion.
Is a Career in Psychiatry Right for You
The students and junior doctors who usually thrive in psychiatry are not just “interested in mental health”. They're comfortable with complexity. They can sit with uncertainty. They want to understand why a person presents the way they do, not just which guideline applies.
Psychiatry is different from psychology because a psychiatrist is a medical doctor. That matters. You diagnose within a medical framework, assess risk, consider physical illness and medication effects, prescribe treatment, and work across hospital, community, crisis, psychotherapy, and specialist diagnostic settings. If you need a clean explanation of that distinction, this guide on the difference between a psychologist and psychiatrist in the UK is useful.
The work suits a particular kind of doctor
If you like immediate procedural feedback, another specialty may suit you better. Psychiatry often rewards slower, more careful thinking. A strong psychiatric assessment can change the direction of a person's life, but it requires patience, structure, and good judgement.
That is especially true in adult ADHD, autism, and broader neurodevelopmental work. These areas demand more than enthusiasm. They require proper developmental history-taking, differential diagnosis, awareness of comorbidity, and enough maturity to avoid overcalling or under-recognising conditions. In practice, some of the most respected consultant careers now sit in precisely these high-demand areas, where diagnostic clarity and communication matter as much as textbook knowledge.
The demand is real, but so is the commitment
There is a strong workforce need. Approximately 10% of consultant psychiatrist roles are unfilled across the UK, and 64% of respondents believed it takes only 5 to 8 years from starting university to become a consultant psychiatrist, which is shorter than the actual route described in the UK study on psychiatry recruitment and training perception (PMC article on consultant vacancies and training misconceptions).
Psychiatry attracts people for humane reasons. They stay in it because the work is intellectually serious, medically grounded, and deeply consequential.
Before you commit, ask yourself three blunt questions:
- Can you tolerate ambiguity well? Many patients won't present with one tidy diagnosis.
- Do you communicate calmly under pressure? Risk, safeguarding, family conflict, and crisis work are common.
- Are you willing to train for the long term? Psychiatry is rewarding, but it isn't a shortcut career.
If the answer is yes, this is one of the few specialties where listening well is not a soft skill at the margins. It is central clinical work.
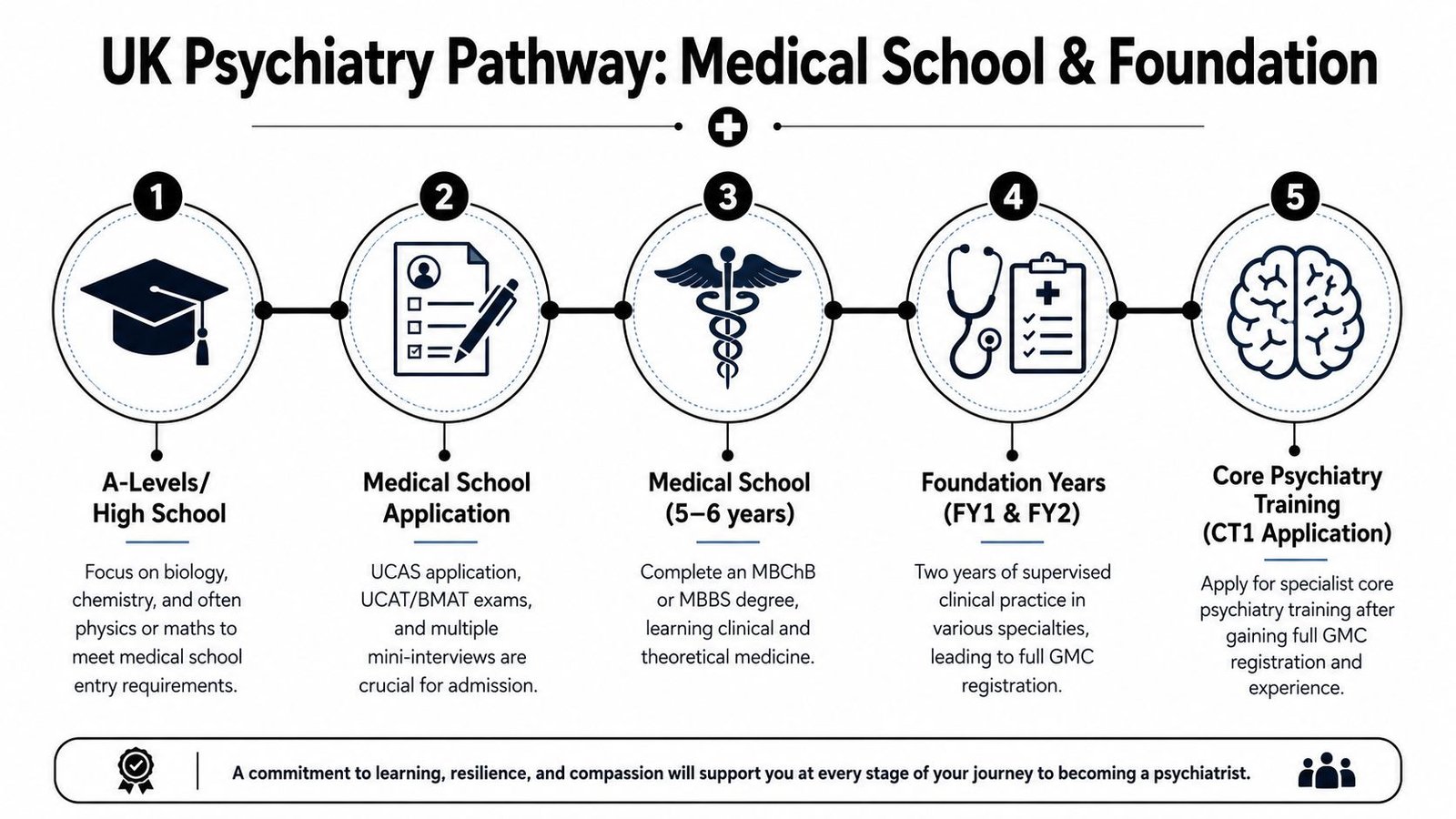
The Core Pathway Medical School and Foundation Years
The route starts in the same place as any other consultant medical career. You need a GMC-recognised medical degree, then the Foundation Programme, and then entry into psychiatry training. The standard UK pathway to consultant psychiatrist status is typically about 13 years from starting medical school, consisting of a 5-year medical degree, 2-year foundation programme, 3 years of core psychiatry training, and 3 years of higher specialist training, as set out by the UK National Careers Service psychiatrist profile.
Medical school comes first
Your first essential step is entry to medicine. That may be a standard undergraduate medical degree or a graduate-entry route if you already hold a prior degree. The exact admissions criteria vary by university, so treat each medical school as its own application project rather than assuming one strategy fits all.
What works early is simple:
- Choose subjects strategically. Medicine usually expects a science-heavy school background.
- Prepare properly for admissions testing. Don't treat UCAT or equivalent selection processes as an afterthought.
- Build evidence of fit for medicine. Reflection matters more than collecting random experiences.
A common mistake is trying to look “psychiatry-focused” too soon. At this stage, your job is to become appointable to medical school and then a solid medical student. Breadth matters. Reliability matters. You can specialise later.
For a practical overview of what the profession looks like day to day, this page on a job as a psychiatrist gives a helpful starting picture.
Use medical school to test, not just admire, psychiatry
Students often like the idea of psychiatry before they've seen enough of it. Clinical practice includes ward rounds, Mental Health Act work, capacity questions, emergency assessments, liaison referrals, and difficult family meetings. You need exposure to know whether you still like it when it becomes real clinical work.
That's why student psychiatry societies, special study modules, and electives matter. They won't substitute for training, but they help you see the actual landscape.
A short visual overview can help fix the sequence in your mind:
Foundation years are where intent becomes visible
FY1 and FY2 are not just a waiting room before specialty training. They are where your habits become obvious. Consultants notice who is safe, organised, reflective, punctual, and kind under strain.
If you think you may want psychiatry, try to secure a psychiatry rotation during foundation if possible. It gives you more than “experience”. It gives you evidence. You can ask for teaching, get involved in a quality improvement project or audit, attend case discussions, and begin to understand the language of psychiatric formulation.
Practical rule: A foundation post in psychiatry is most valuable when you use it to build relationships, write reflections well, and learn how psychiatric teams make decisions.
What doesn't work is drifting through foundation assuming enthusiasm alone will carry you. By the time CT1 applications open, panels want signs that you understand the specialty as it is practised, not as you imagined it from lectures.
Entering Psychiatry Training Core and Higher Specialisation
After foundation, you enter the specialist pathway. At this point, the broad interest in mental health must evolve into disciplined training. Psychiatry in the UK is a six-year post-foundation programme, split into three years of core training (CT1 to CT3) and three years of higher training (ST4 to ST6). Passing all parts of the MRCPsych by the end of CT3 is mandatory for progression to higher training, as set out by the Royal College of Psychiatrists pathway guidance.
Core training is where you learn to think like a psychiatrist
CT1 to CT3 gives you the foundations. You rotate through different settings and patient groups, learn assessment structure, risk formulation, legal frameworks, diagnostic reasoning, psychopharmacology, and multidisciplinary working. This is also the stage where many trainees discover whether they are more drawn to acute work, psychotherapy-informed practice, community complexity, or a specialist niche.
The table below is the simplest way to hold the pathway in mind.
| Stage | Typical Duration | Key Objective / Milestone |
|---|---|---|
| Foundation Programme | 2 years | Build broad clinical competence and full GMC registration |
| Core Psychiatry Training CT1 to CT3 | 3 years | Gain psychiatric foundations across posts and pass MRCPsych |
| Higher Psychiatry Training ST4 to ST6 | 3 years | Develop specialty-level expertise and prepare for consultant practice |
| CCT and Specialist Register | End point | Complete training and become eligible for substantive consultant roles |
MRCPsych is not just an exam hurdle
Many juniors approach MRCPsych as if it were a separate academic nuisance. That's the wrong mindset. The exam tests whether your knowledge is developing in step with practice. If your revision is detached from patients, tribunals, formulations, prescribing, supervision, and psychotherapy exposure, it becomes harder.
When trainees ask me what helps, I usually say this:
- Study early and steadily. Last-minute panic revision rarely works well in psychiatry because the material is broad and conceptual.
- Tie revision to cases. If you see the condition, medication, or framework in clinic, revise it that week.
- Use question practice intelligently. Don't just chase scores. Work out why your thinking went wrong.
- Protect supervision time. Good supervisors sharpen clinical reasoning and often rescue trainees from avoidable mistakes.
If you're already thinking ahead about structured revision resources, especially for high-stakes exams and board-style preparation habits, this guide on preparing for your psychiatry boards is worth reviewing for study discipline and exam planning.
Higher training is where your future shape appears
ST4 to ST6 is where your consultant identity starts to become visible. The exact route depends on your chosen higher specialty, but this is the point at which your day-to-day work, case mix, supervision, and longer-term opportunities begin to align.
Some doctors choose general adult psychiatry and later develop a subspecialist interest. Others are drawn earlier to old age, forensic, child and adolescent, liaison, medical psychotherapy, or intellectual disability pathways. If you're interested in adult ADHD, autism, and neurodevelopmental assessment, your best route often involves developing strong core skills in differential diagnosis, developmental history, comorbidity assessment, and complex formulation.
That kind of work isn't superficial diagnostic sorting. It requires you to distinguish between overlapping presentations such as trauma, mood disorder, anxiety, personality difficulty, substance use, sleep disturbance, and genuine neurodevelopmental conditions. In good specialist practice, the assessment is careful, evidence-based, and medically integrated.
What selection panels notice later on
By the time you are moving through training, exam success alone doesn't make you stand out. Appointable future consultants usually show a pattern:
- They document clearly. Poor records damage good clinical thinking.
- They formulate, not just list symptoms. Senior psychiatry depends on synthesis.
- They work well with teams. Nurses, psychologists, occupational therapists, GPs, and social care colleagues all matter.
- They choose niches with substance. Neurodevelopmental work is attractive, but only if you build proper expertise rather than collecting labels.
If you're exploring where UK psychiatrist careers can develop across different settings, this overview of psychiatrist jobs in the UK gives a useful sense of the broader picture.
The best trainees don't rush to look specialist. They become dependable first, then distinctive.
Building a Standout Application and Nailing the Interview
A surprising number of applicants think passing exams and turning up with enthusiasm should be enough. It isn't. Selection panels want evidence that you understand the work, can reflect on experience, and will be safe to train.

Build a portfolio with a theme
A scattered portfolio often signals a scattered candidate. A better approach is to build around a credible thread. That thread might be acute psychiatry, medical education, psychotherapy, liaison work, or neurodevelopmental assessment. The point isn't to pretend you are already a specialist. The point is to show consistent interest and useful initiative.
Good evidence usually includes a mixture of the following:
- Clinical audit or quality improvement: Something completed, not half-started.
- Teaching: Even small-group teaching counts if you can reflect on it properly.
- Psychiatry-specific exposure: Taster weeks, electives, foundation placements, supervised clinics.
- Reflective maturity: Panels can tell when your portfolio is a box-ticking exercise.
Interview performance is mostly about judgement
The strongest candidates don't sound rehearsed. They sound thoughtful. They answer directly, then show that they understand nuance, uncertainty, patient safety, and team dynamics.
Senior advice: Don't try to sound impressive. Try to sound trainable, honest, and clinically sensible.
For practice, mock interviews with consultants or registrars are still best because they can challenge your reasoning, not just your wording. If you also want a structured way to rehearse common interview responses out loud, an AI interview assistant can help you spot weak phrasing, rambling answers, and gaps in clarity before your interview.
What usually weakens an otherwise good applicant
Three patterns come up repeatedly.
- Overclaiming interest: Saying psychiatry is your passion without evidence behind it.
- Thin reflection: Describing an experience without showing what you learned from it.
- Poor understanding of the specialty: Especially around risk, teamwork, and the realities of mental health services.
A panel can teach knowledge gaps. It can't easily teach humility, integrity, and self-awareness. Those are the qualities that often separate the appointable candidate from the merely enthusiastic one.
Alternative Routes and Pathways for IMGs
For International Medical Graduates, the route is absolutely possible, but it is less forgiving if you don't understand the system early. Most problems I see are not caused by lack of ability. They come from avoidable confusion about registration, evidence of competence, and where non-UK experience fits into UK recruitment.
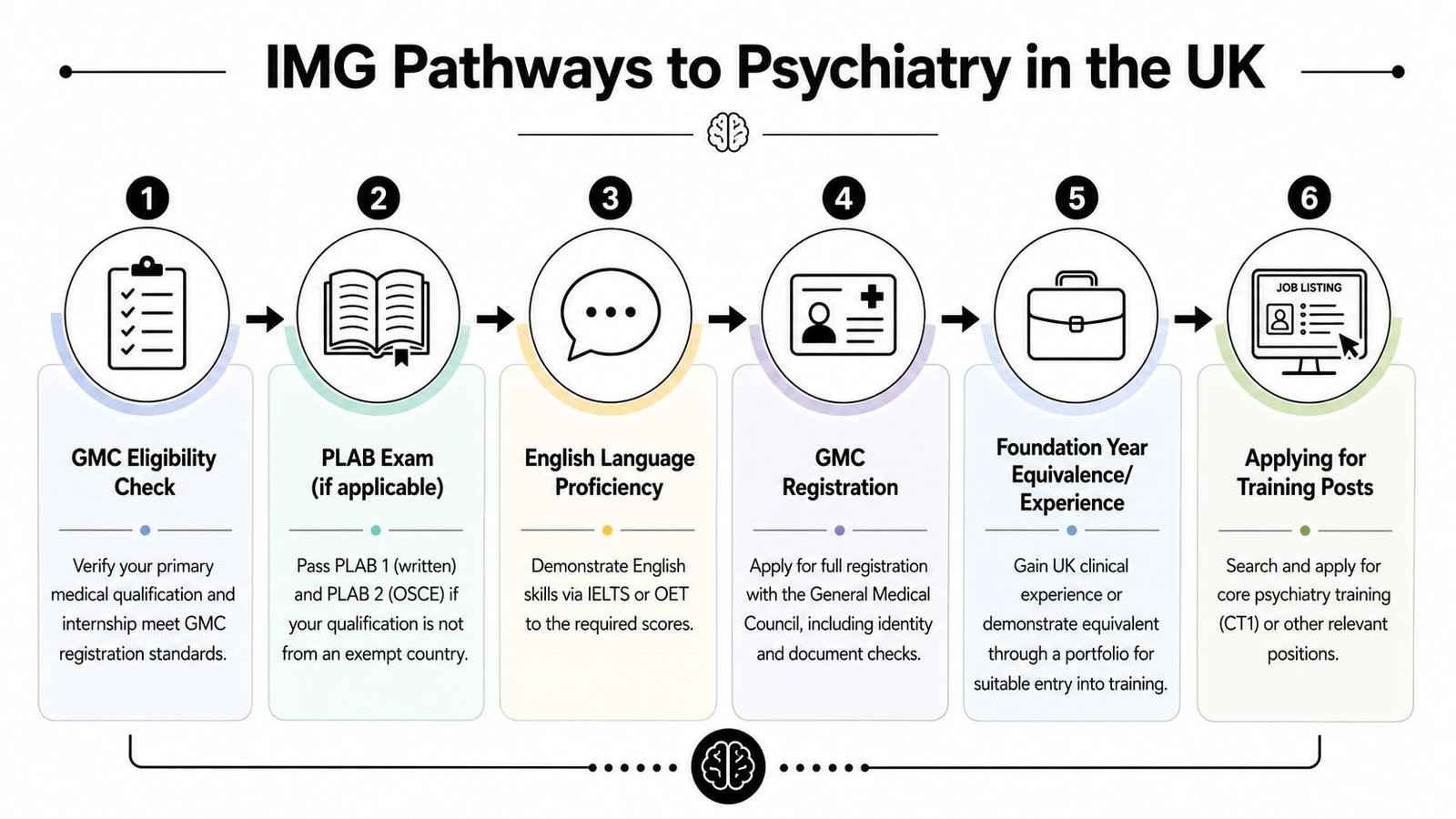
Registration comes before specialty ambitions
For IMGs, the practical sequence often starts with GMC registration, and for many doctors this involves the PLAB route. One of the key complications is the uncoupled nature of psychiatry training, meaning completion of core training does not automatically secure a higher training post. Strong portfolio evidence and MRCPsych progress matter at several stages, as discussed in this UK psychiatry IMG pathway video overview.
That means you should think in layers:
- Can you obtain the right GMC registration route?
- Can you show English language readiness and clinical communication at UK standard?
- Can you demonstrate equivalent foundational competence for training entry?
- Can you compete within national recruitment once eligible?
CREST and equivalent competence matter more than many IMGs expect
A common misunderstanding is that prior psychiatric experience alone will automatically make UK training entry straightforward. It often won't. Recruitment is competency-based. Panels need evidence that your prior work maps onto what UK training expects.
That is where documentation matters. If you need to use a competence form such as CREST or show equivalent readiness for specialty training, the quality of that evidence can make the difference between progress and delay.
Here is what usually helps most:
- Get your paperwork right early. Missing signatures, unclear dates, and inconsistent job descriptions create avoidable problems.
- Seek UK clinical exposure if possible. Even a limited period can help you understand expectations around notes, handover, escalation, and MDT culture.
- Don't assume seniority abroad translates neatly. UK assessors still need evidence in their own framework.
- Prepare for repeated competition points. Entry into training is one hurdle. Progression later is another.
There is more than one workable route
Some IMGs enter directly into training once registration and competence evidence are in place. Others first take non-training posts in psychiatry, build UK experience, strengthen references, and then apply. That second route can be very sensible, especially if you want time to understand the NHS, improve portfolio evidence, and adapt to interview style.
Many IMGs succeed because they stop trying to decode the whole UK system at once and focus on the next document, the next competency, and the next safe decision.
What doesn't work is rushing into applications with partial understanding. Psychiatry in the UK rewards careful preparation. That is true for everyone, but IMGs feel the consequences of poor preparation more quickly.
Life as a Consultant and The Future of Psychiatry
By the time you reach consultant level, the job becomes broader and more interesting. You are no longer just delivering individual assessments under supervision. You are shaping care pathways, making final clinical decisions, leading teams, supervising trainees, contributing to service design, and carrying a higher level of responsibility for complexity and risk.
In consultant practice, no two weeks are identical. One day may involve diagnostic clarification, medication decisions, multidisciplinary planning, and supervision. Another may be dominated by report-writing, second opinions, family meetings, or service leadership. That variety is one reason many psychiatrists stay engaged with the work for decades.
High-demand specialist practice is changing the field
One of the clearest examples of psychiatry's future is the growth of rigorous consultant-led work in adult ADHD, autism, and broader mental health assessment. These clinics meet a real need, but they also expose a hard truth. Good neurodevelopmental assessment is difficult. It requires proper structure, developmental detail, careful ruling in and ruling out, and enough experience to avoid simplistic labelling.
That's why careers shaped by senior consultants working in neurodevelopmental conditions and personality complexity are so instructive. They show that psychiatry can be both highly specialised and thoroughly person-centred. In those settings, the consultant is not just diagnosing. They are integrating developmental history, current impairment, comorbidity, treatment planning, and communication with clarity.
A good endpoint is worth the long road
Students often fixate on whether the training is long. It is. But the better question is whether the endpoint is professionally satisfying. For many psychiatrists, it is.
Consultant life can give you a combination that few specialties offer:
- Clinical depth
- Meaningful longitudinal work with patients
- Teaching and leadership
- Room to develop niche expertise
- Flexible career models across NHS and independent practice
If you're also thinking pragmatically about consultant earnings and how pay evolves across the profession, this guide on how much psychiatrists make is a sensible companion read.
The strongest consultant careers usually aren't built by chasing prestige. They're built by becoming trusted in an area where patients need excellent judgement.
Frequently Asked Questions about a UK Psychiatry Career
How long does it take to become a consultant psychiatrist in the UK
The standard route is typically about 13 years from starting medical school, based on a medical degree, foundation training, core psychiatry training, and higher specialist training. Some doctors take a little longer or slightly different routes depending on prior degrees, intercalation, time out, or alternative entry pathways.
Is psychiatry a good specialty for someone interested in ADHD and autism
Yes, but only if you want to approach those conditions with proper clinical discipline. Adult ADHD and autism work is rewarding, but it is not lightweight practice. You need to enjoy detailed assessment, developmental history, differential diagnosis, and careful report writing.
Do I need MRCPsych to progress
Yes. Passing MRCPsych by the end of core training is required for progression into higher psychiatry training.
Can I work in psychiatry before entering formal training
Yes. Many doctors work in psychiatry in non-training roles before entering CT1, and that can be particularly useful for gaining experience, references, and portfolio evidence. For IMGs, this can also help bridge into UK practice more smoothly.
Is psychiatry mainly talking and paperwork
No. Communication and documentation are central, but psychiatry is still medicine. You assess risk, diagnose within a medical framework, prescribe, manage complexity, and make decisions with major consequences for safety, functioning, and quality of life.
Is work-life balance better than in other specialties
It can be, depending on your post, setting, and boundaries. Psychiatry often offers a more sustainable rhythm than some acute procedural specialties, but emotional load, administrative burden, and service pressure are real. Good supervision, team culture, and sensible career choices matter.
If you're exploring assessment, diagnosis, or consultant-led support for adult ADHD, autism, and wider mental health concerns, Insight Diagnostics Global offers online and face-to-face assessments for adults aged 18 and over, with structured evaluations, clear reports, and follow-up options delivered by psychiatrists on the GMC Specialist Register.